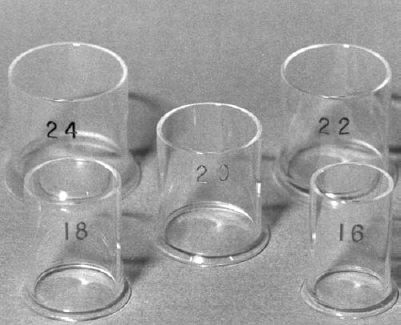
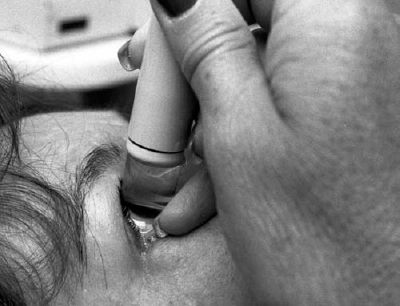
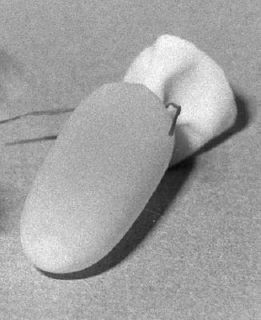
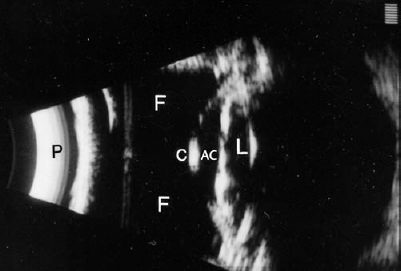
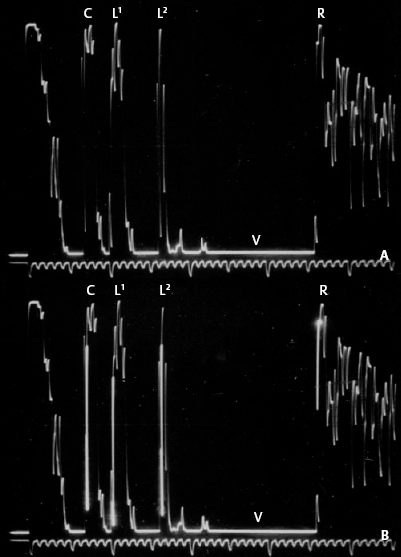
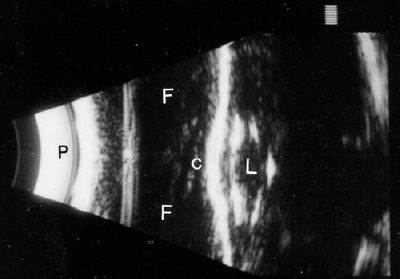
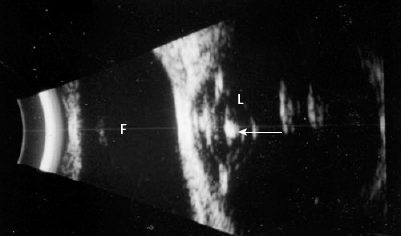
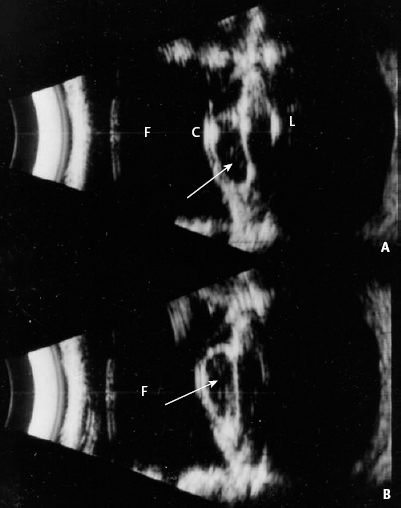
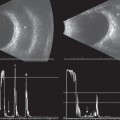
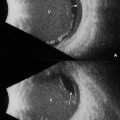
2 Echographic evaluation of the anterior segment using an immersion or water bath technique can be a useful tool. When anterior segment pathology is noted or suspected and slit lamp and gonioscopic evaluation do not allow for adequate visualization of the cornea, anterior chamber, iris, iris angle, ciliary processes, and the anterior surface of the lens, immersion ultrasound can be used. Conventional contact B-scan is of little use in evaluating anterior eye structures because of the required contact of the probe to the globe surface. Typically, there is a 5-mm area directly in front of the probe known as the “dead zone” where imaging is not possible. It is, however, possible to create a stand-off so the dead zone does not impede imaging. This can be accomplished using scleral shells that are commercially available. These shells are small, plastic cups that come in different diameter widths to accommodate different eye and lid fissure sizes. They fit beneath the lids and can be filled with fluid to create the necessary stand-off. The probes can either be placed on top of the shell or immersed into the fluid-filled chamber. For some patients who have had recent surgery or trauma, inserting an inflexible scleral shell beneath the lids is not recommended. For these patients, a modified immersion technique can be used. To create a stand-off for this technique, the finger of a glove can be used to create a fluid-filled “balloon.” This soft balloon can then be placed on the lids or the globe to evaluate anterior eye structures. The resolution of the images will not be as clear as those obtained with regular immersion techniques, but some useful information can be obtained. Over the last decade, higher-resolution equipment has emerged in ophthalmology. This equipment provides stunning images of the cornea, iris, lens, and ciliary body and has increased our ability to study anterior segment tumors, the mechanisms of glaucoma, intraocular lens positioning, corneal changes, and traumatized eyes. The ultrasound frequency of current contact B-scan transducers is around 10 MHz. The new generation, higher-resolution probes have frequencies that range from 20 to 100 MHz. The 20 MHz probe produces an image that is 10-mm wide, 12-mm deep, and provides resolution in the 75-μm range. The transducer can be immersed into a water bath or a fluid-fill tonometer cover can be placed over the exposed piezoelectric crystal. The 50- to 100-MHz probes, also known as UBM (ultrasound biomicroscope), produce a 4-mm depth of penetration and provide resolution in the 50-μm range. These transducers work best when immersed in a water bath. Transverse, longitudinal, and axial scans can be performed using these probes; however, the marker orientations are somewhat different than those used for screening the posterior segment. Typically, the marker is directed toward the corneal limbus and pupil in longitudinal scans; however, for anterior segment evaluation using longitudinal scans the marker is directed away from the corneal limbus, toward the sclera. The designation for the marker using transverse scans is in any direction, but the recommended scanning procedure should be performed in a clockwise fashion. We have expanded this chapter to include images using probes from various frequencies. Each probe (10, 20, or 50–100 MHz) continues to provide useful echographic information with regard to anterior segment structures. It is the responsibility of the echographer to decide which frequency will provide the best information for the exam indication. Byrne SF, Green RL. Ultrasound of the Eye and Orbit. St. Louis: CV Mosby Yearbook; 1992 Ossoinig KC. Standardized echography: basic principles, clinical applications and results. Int Ophthalmol Clin 1979;19(4):127–210 Pavlin CJ, Foster FS. Ultrasound Biomicroscopy of the Eye. New York: Springer-Verlag; 1995 Pavlin CJ, Harasiewicz K, Sherar MD, Foster FS. Clinical use of ultrasound biomicroscopy. Ophthalmology 1991;98(3):287–295 Figure 2–1 Immersion shells. Set of scleral shells for immersion technique/water bath. The numbers represent the diameter in millimeters. Figure 2–2 B-scan. Immersion shell in correct position; fluid overflows shell to maintain fluid/probe contact. Figure 2–3 Immersion A-scan. Because the probe is small and fits into all sizes of shells, it is not necessary to fill the scleral shells completely. Figure 2–4 Modified immersion. The finger of a latex glove if filled with water and tied with a rubber band to resemble a small balloon. Figure 2–6 Immersion A-scan. (A) Axial image. A double-peaked spike is produced by the cornea (C). High spikes are produced from the anterior and posterior lens surfaces (L1, L2). The normal vitreous (V) produces a baseline, and a maximally high spike is produced from the retina (R). (B) Cursors are placed at the correct surfaces for measurement of the anterior chamber, lens thickness, and total axial length. Figure 2–7 Modified immersion. C, cornea; F, fluid in latex glove; L, lens; P, probe. Figure 2–8 Lens/cataract. AC, anterior chamber; arrow, lenticular opacities; C, cornea; F, fluid; L, lens. Figure 2–9 Lens/membranous cataract. AC, anterior chamber; C, cornea; F, fluid; L, membranous cataract. Figure 2–11 Anterior chamber cyst. (A) Axial immersion. Arrow, anterior chamber cyst; C, cornea; F, fluid; L, lens. (B) Immersion performed directly over cyst (arrow). Figure 2–12 Anterior chamber/hyphema. Axial modified immersion. Arrow, hyphema; C, cornea; F, fluid in finger of glove; L, lens.
Anterior Segment Evaluation
 Suggested Readings
Suggested Readings




Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


