APPROACH TO HIGH INTESTINAL OBSTRUCTION IN A NEONATE
Namita Singh, Akriti Gujral
Fig. 7.4.1.1Midline epigastric scan showing symmetrically thickened hypoechoic muscle of the pylorus with central echogenic mucosa.
Clinical history
A one-month-old infant was brought to the emergency with projectile nonbilious vomiting. The mother complained that the baby begins to vomit 30–45 min after feeding. The baby remains hungry and wants to be fed very often. On examination, the baby is lethargic, skin is clammy and the fontanelles are depressed.
Radiological study
Ultrasonography (USG) of abdomen: Usually performed in the right lateral decubitus position to allow fluid to distend the antral region.
Observation
USG reveals a target sign seen as a thickened hypoechoic muscle mass of the hypertrophied pylorus surrounding the central echogenic thin mucosal line.
Diagnosis
Congenital hypertrophic pyloric stenosis
This is a common cause of high intestinal obstruction in a neonate. It is usually seen in the first-born male infant. Age of presentation can be any time between 5 days and 5 months. There is hypertrophy of the pylorus, resulting in difficulty in passing of chyme forward leading to a gastric outlet obstruction. The infant presents with nonbilious projectile vomiting especially after a feed. The baby is hungry after vomiting and wants to be fed again. Repeated episodes of vomiting can result in dehydration, malnutrition and failure to gain weight.
Imaging
USG: This is the preferred imaging modality as it is noninvasive and does not pose any radiation hazard. USG is performed with a 6–10 MHz linear probe. Fluid distention of the stomach can aid in visualization of the pylorus. A sausage-shaped mass with a total thickness of more than 14 mm and length in excess of 16 mm with each wall measuring at least 4 mm is indicative of congenital hypertrophic pyloric stenosis.
Analysis and interpretation through logical and informed approach
Vomiting in a neonate can be due to innocuous conditions like gastro-oesophageal reflux or more sinister conditions that result in intestinal obstruction. Unlike adults in whom intestinal obstruction is divided into small and large bowel obstruction, in neonates it is classified as high and low intestinal obstruction. This is because haustra are not well developed in the large bowel in a neonate; hence, small bowel cannot be differentiated from the large bowel on plain radiography. High obstruction being due to lesions proximal to the ileum and low obstruction involving distal ileum and colon.
The first radiological investigation of a neonate with suspected intestinal obstruction should be an abdominal radiograph. If the radiograph shows less than four (air-filled) bowel loops, then a high intestinal obstruction would be suspected and a USG abdomen or barium upper GI study would be indicated. In case four or more (air-filled) bowel loops are present, then the infant is likely to have a low intestinal obstruction in which case a barium enema would be considered as the next investigative step.
The bowel gas pattern gives a clue to the level of obstruction:
a) One gas bubble suggests gastric outlet obstruction.
b) Two gas bubbles (double bubble) is indicative of duodenal obstruction.
c) Three, that is, triple bubble is indicative of high intestinal obstruction, for example, jejunal atresia.
d) Four or more gas bubbles is indicative of low intestinal obstruction.
Investigation in high intestinal obstruction could include plain radiography, USG, colour Doppler, barium meal upper GI series and CT abdomen.
High intestinal obstruction in a neonate can be caused by:
a) Anomalies of the stomach: For example, microgastria, congenital hypertrophic pyloric stenosis, antral webs, ectopic pancreatic tissue in the pyloric antrum resulting in partial obstruction.
b) Anomalies of the duodenum:
a. For example, duodenal obstruction due to intrinsic causes such as duodenal atresia leading to a complete obstruction or duodenal webs leading to an incomplete obstruction.
b. Duodenal obstruction due to extrinsic causes, for example, annular pancreas, malrotation or SMA (SMA syndrome).
c) Anomalies of the jejunum: Jejunal atresia.
Other Causes of High Intestinal Obstruction in a Neonate:
Diagnosis
Clinical and Radiological Findings
Image
Duodenal atresia
Duodenal atresia can result in bilious or nonbilious vomiting in the first 24 hours after birth.
The atresia is usually located distal to the ampulla of Vater. In complete atresia, no gas will pass distal to the duodenum and there will be collapse of the bowel loops.
Associated with polyhydramnios and VATER anomalies (vertebral defects, anal atresia, tracheo-oesophageal fistula with oesophageal atresia, radial and renal anomalies)
Plain radiograph shows the double bubble sign with no distal gas in the abdomen. The double bubble sign represents dilatation of the stomach and duodenum.
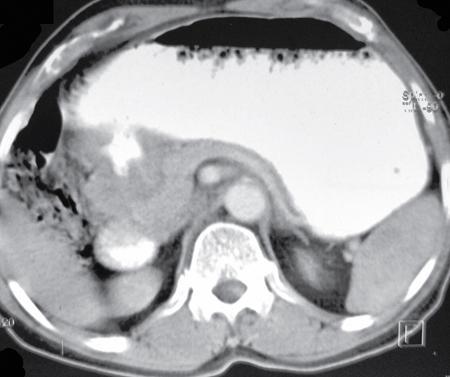
Note: When oesophageal atresia is associated with duodenal atresia, no air enters the stomach and the child presents with a large opaque midabdominal mass (representing the stomach).
Fig. 7.4.1.2Radiograph of the abdomen showing double bubble sign due to air distending the stomach and duodenum with no gas distal to the duodenum.
Annular pancreas
It can present in infancy or in fourth/fifth decade of life. Only one-third of patients with annular pancreas become symptomatic. Symptoms depend upon the amount of luminal obstruction caused and consists of bilious vomiting, pain abdomen and refusal to feed. The bilious vomiting is due to duodenal obstruction.
It is associated with polyhydramnios, Down’s syndrome, oesophageal and duodenal atresia, imperforate anus and Meckel’s diverticulum.
Plain radiograph shows a double bubble sign due to dilatation of the duodenum and stomach.
USG: Antenatal sonology detect distended stomach and duodenum in a patient presenting with polyhydromnios as seen in the adjacent image
Fig. 7.4.1.3Antenatal USG reveals double bubble sign with stomach and duodenum distended with fluid.
Malrotation
Caused by abnormal position of the DJ junction which can lead to midgut volvulus.
The DJ junction is normally sited to the left of the left vertebral pedicle at the same superoinferior level as the pylorus. Majority (80%) of the intestinal malrotation cases present within a month after birth.
The usual symptom is bilious vomiting.
Radiological signs of malrotation are:
• abnormal position of the DJ junction to the right of the vertebral column.
• the proximal jejunal loops will be located to the right side.
• the cecum may be located in the midabdomen or left upper quadrant.
Fig. 7.4.1.4Plain radiograph of a neonate showing abnormally positioned small bowel loops to the left and large bowel to the right side of the abdomen.
Midgut volvulus
Though it can occur at any age but it is most common in the neonate who has an associated GI malrotation.
In midgut volvulus, twisting of the intestine occurs. Apart from vomiting and abdominal distention, these patients may show evidence of hemodynamic collapse. If the volvulus has caused bowel ischaemia there can be presence of haematochezia as well.
Plain radiograph may show few air fluid levels or can be normal.
Barium study will show an abnormal location of the duodenojejunal junction to the right of the vertebral column at the level of the pylorus, indicating malrotation of the gut.
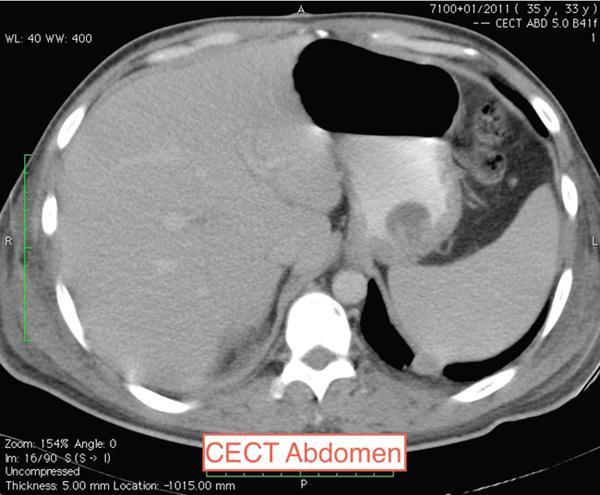
Abdominal Doppler can reveal the SMV lying in front of or to the left of the SMA indicating an inverse relationship of these vessels. CT abdomen can show clockwise twisting of the mesenteric vessels – the whirlpool sign.
Fig. 7.4.1.5CECT in a patient with midgut volvulus showing the whirlpool sign (clockwise twisting of the mesenteric vessels).
Jejunal atresia
Proximal jejunal atresia causes intestinal obstruction in the new born.
It is usually caused by an intrauterine mesenteric vascular insult.
Prenatal Parvovirus B-19 infection has also been implicated.
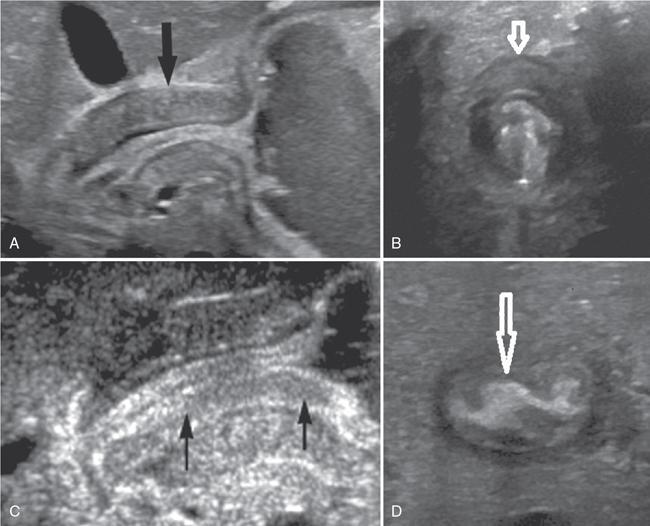
Prenatal USG reveals dilated bowel loops.
After birth, plain radiograph reveals the triple bubble sign. The three bubbles represent air in stomach, duodenum and proximal jejunal loops. The jejunum proximal to atresia gets massively dilated. Triple bubble becomes visible on erect abdominal radiograph 4 h after birth after swallowed air reaches the jejunum. There may be accompanying small unused colon which can be seen on a barium enema.
Fig. 7.4.1.6(A) Prenatal USG: The dilated stomach was followed into the dilated duodenum, which continued into the proximal dilated jejunum that tapered at the site of atresia. (B) Case of jejunal atresia, postnatal radiograph showed dilated proximal bowel loops with unused small colon showing minimal luminal air. (C) Barium enema showing microcolon in another case of jejunal atresia.
7.4.2
APPROACH TO PHARYNGEAL AND OESOPHAGEAL POUCHES AND DIVERTICULA
Debraj Sen
Fig. 7.4.2.1Barium swallow in a 50-year-old male with history of progressive dysphagia of one-year duration. Source: (Image courtesy Dr Vijinder Arora, Nijjar Scan & Diagnostic Centre, Amritsar, India.) Radiological Technique: Barium swallow (barium pharyngography).
Observations
A barium-filled outpouching is seen posterior to the cervical oesophagus, with the neck of the pouch at the level of C5–C6 (just cranial to the anticipated position of the cricopharyngeus muscle).
Principal Diagnosis: Zenker’s diverticulum.
Pharyngeal/oesophageal pouches and diverticula are mucosal protrusions through weaknesses in the muscular pharyngeal wall. Pouches are transient and diverticula are permanent. Based on their aetiology, they can be classified as pulsion, traction or developmental. Based on location, cranial to caudal, these are:
1. Pharyngocele
2. Zenker’s diverticulum
3. Lateral pharyngeal pouches and diverticula
4. Lateral cervical oesophageal pouch and diverticulum (Killian–Jamieson diverticula)
Upper one-third
5. Traction diverticula
6. Developmental diverticula
7. Intramural
Middle one-third
8. Epiphrenic
9. Mallory–Weiss syndrome (mucosal tears)
10. After Heller’s myotomy
Lower one-third
Diagnosis
Imaging and Clinical Features
Images
Traction diverticulum
• This is an acquired condition due to adhesions formed with subcarinal or perihilar lymph nodal disease (like tuberculosis).
• They usually occur in the midoesophagus, triangular in shape with pointed tip and a wide neck.
• Traction diverticulum tends to empty when oesophagus is collapsed as walls have muscle.
• Similar lesion may be seen due to oesophageal dysmotility (pulsion diverticulum).
Fig. 7.4.2.2Barium oesophagogram showing a midoesophageal traction diverticulum.
Multiple diverticula
• Multiple pulsion diverticula.
• Almost all patients have spastic oesophageal spasm or oesophageal dysmotility.
• They have a wide neck with smooth rounded contours.
• As the walls are devoid of muscle, they tend to remain filled with barium after passage of the barium bolus.
• Most patients have evidence of oesophageal dysmotility.
• They tend to remain filled with barium as they lack muscle in the wall.
• May be mistaken for hiatal hernia (important to look for gastric folds).
Fig. 7.4.2.4Barium oesophagogram showing an epiphrenic diverticulum.
7.4.3
APPROACH TO OESOPHAGEAL DYSPHAGIA
Debraj Sen
Clinical history
Fifty-year-old male with history of progressive dysphagia of one-year duration.
Observations
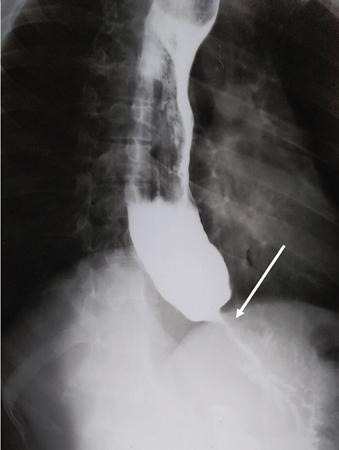
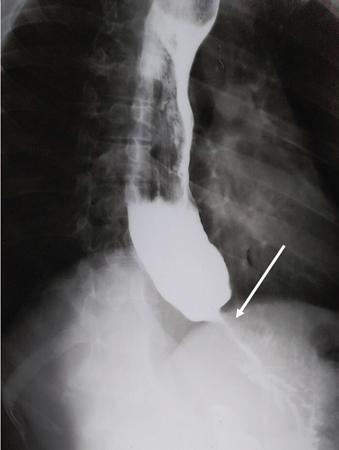
Upright oblique anteroposterior image reveals a markedly dilated barium-lined oesophagus showing food residue, mottled gas and an air-fluid level. The dilated oesophagus shows smooth distal tapering to a ‘bird beak’-like appearance below the diaphragm (arrow). On fluoroscopy, primary oesophageal peristalsis was absent.
Principal Diagnosis: Achalasia cardia.
Differential diagnosis
1. Presbyoesophagus
2. Carcinoma
3. Scleroderma
4. Oesophagitis with stricture
Fig. 7.4.3.1Barium swallow of the patient. Radiological technique: Barium swallow (barium oesophagography).
Diagnosis
Imaging Findings
Image
Presbyoesophagus
Barium oesophagogram in an 80-year-old male, showing a dilated oesophagus with hold-up of barium, tertiary contractions and partial relaxation of the lower oesophageal sphincter.
The oesophageal calibre <4 cm and there is no ‘bird’s beak’ appearance of distal oesophagus with intermittent passage of barium.
Barium oesophagogram in a 50-year-old male patient showing asymmetric mural thickening, ‘shouldering’, mucosal irregularity with a long segment of luminal narrowing (arrow). There is upstream hold-up of contrast and dilatation of the oesophagus.
In case of gastric carcinoma with extension into GE junction, associated fundic mural thickening and mucosal irregularity may be seen.
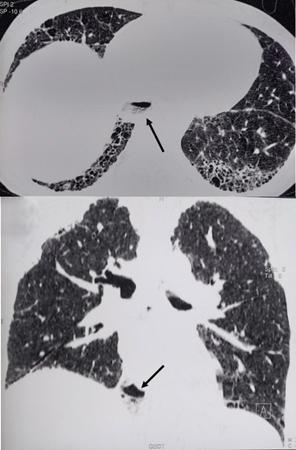
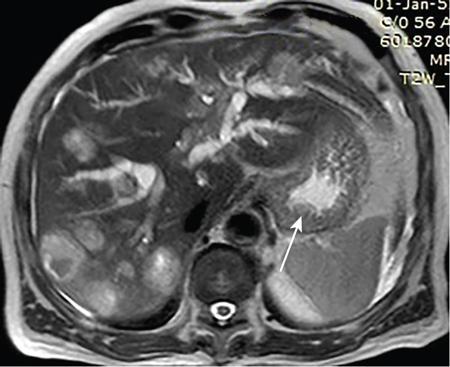
High-resolution computed tomography (HRCT) lung (axial and coronal reformatted images) of a 32-year-old female patient shows a dilated patulous distal oesophagus and gastro-oesophageal junction (arrow) and features of Usual interstitial pneumonia (UIP) pattern of interstitial lung disease.
Fig. 7.4.3.4HRCT images showing dilated patulous GE junction and UIP pattern of interstitial lung disease.
7.4.4
APPROACH TO OESOPHAGEAL LUMINAL NARROWING
Debraj Sen
Clinical history
Fifty-year-old male with history of progressive dysphagia of six months’ duration associated with significant weight loss.
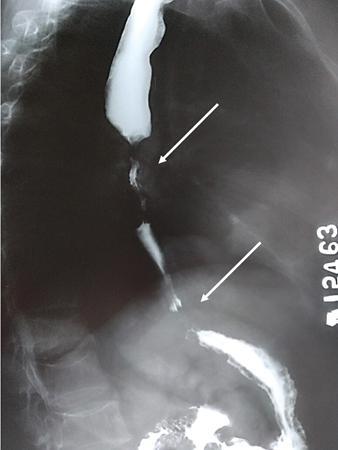
Barium oesophagogram showing a long segment of asymmetric mural thickening, ‘shouldering’ and mucosal irregularity with luminal narrowing (arrow) in the distal oesophagus and gastro-oesophageal junction, producing a ‘rat-tail’ appearance. There is upstream hold-up of contrast and dilatation of the oesophagus producing the ‘pseudoachalasia’ appearance.
Ancillary findings (of pseudoachalasia) – Decreased or absent peristalsis with luminal diameter usually <4 cm; length of narrowed segment is >3.5 cm.
Based on the frequency of occurrence, causes of oesophageal luminal narrowing may be classified as intrinsic or extrinsic. Extrinsic luminal narrowing can be due to left main bronchus, aortic arch, aberrant right subclavian artery, aneurysm, mediastinal lymph nodes, etc.
Causes of intrinsic luminal narrowing may be classified as under:
• Oesophageal carcinoma
• Stricture (ingestion of chemicals, drugs, postradiation, postsurgical)
• Intramural benign oesophageal tumours
Common
• Thrombosed oesophageal varix
• Inflammatory polyp
• Papilloma
Less common
• Fibrovascular polyp
• Oesophageal metastases and lymphoma
• Oesophageal adenoma
Rare
Fig. 7.4.4.1Barium swallow of the patient.
Diagnosis
Imaging and Clinical Features
Images
Achalasia cardia
• Occurs due to decrease in ganglion cells in Auerbach’s myenteric plexus with loss of primary peristalsis and concomitant impaired relaxation of the lower oesophageal sphincter, resulting in a dilated oesophagus (megaoesophagus).
• Smooth, symmetrical and conical (‘V’-shaped) tapering of the distal oesophagus up to the GE junction producing a ‘bird’s beak’ appearance (arrow) with hold-up of barium.
• Luminal diameter is usually >4 cm and length of narrowed spastic segment is <3.5 cm.
• A long segment of luminal narrowing seen in the mid- and distal oesophagus with ‘shouldering’ (arrows) and proximal hold-up of contrast.
Fig. 7.4.4.3Barium oesophagogram showing carcinoma mid- and distal oesophagus.
Diffuse oesophageal spasm
• Patients usually >50 years of age, and present with intermittent chest pain and/or dysphagia.
• Oesophageal motility disorder in which there are multiple spontaneous and uncoordinated oesophageal contractions.
• On barium swallow, uncoordinated contractions are seen obliterating the lumen in the distal two-thirds of the oesophagus producing a classic ‘corkscrew’ appearance. Note that there is no mucosal irregularity, ‘shouldering’.
Fig. 7.4.4.4Barium oesophagogram showing ‘corkscrew’ appearance in diffuse oesophageal spasm.
Postsurgical stricture
• Short segment oesophageal anastomotic site stricture in the middle one-third following surgery for oesophageal carcinoma.
• Multiple smoothly marginated linear and serpentine submucosal impressions in the lower oesophagus. Note that there is no mucosal irregularity or ulceration. The size and appearance of oesophageal varices change with respiration and patient’s position.
• ‘Uphill’ varices are usually seen in the lower one-third of the oesophagus in the portal hypertension.
• ‘Downhill’ varices are typically seen in SVC obstruction and involve the upper and middle one-third of the oesophagus.
Fig. 7.4.4.6Barium oesophagogram showing ‘uphill’ oesophageal varices. Source: (Image courtesy Dr Vijinder Arora, Nijjar Scan & Diagnostic Centre, Amritsar, India.)
Varicoid carcinoma oesophagus
• Multiple linear and tortuous serpentine submucosal filling defects in the upper and middle two-thirds of the oesophagus simulating ‘downhill’ varices. Note, however, that there is mucosal irregularity and ulceration. These filling defects also do not change in appearance with respiration or position.
• Varicoid carcinoma is not a separate histopathological entity but is an appearance that is seen in oesophageal carcinoma that disseminates via vessels and lymphatics to the submucosa.
• A similar appearance may also be seen in lymphoma and metastases.
Fig. 7.4.4.7Barium oesophagogram showing varicoid pattern of carcinoma oesophagus. Source: (Image courtesy Dr Vijinder Arora, Nijjar Scan & Diagnostic Centre, Amritsar, India.)
7.4.5
APPROACH TO GASTRIC FILLING DEFECTS
Sehajbir Kaur Pannu
Clinical history
Fifty-year-old lady with vague upper abdominal discomfort.
Barium study shows large filling defect in the antrum forming acute angles with the wall. Undulating contour is seen along greater curvature with ulceration of overlying mucosal irregularity.
CECT shows a large lobulated mass involving lesser curvature and antrum with marked wall thickening along distal greater curvature.
Diagnosis
Carcinoma stomach.
Differential diagnosis of gastric masses
Gastric carcinoma
95% are adenocarcinomas.
Mucosal lesion – erosion and ulceration common; perigastric tissue invasion may be seen; lymphadenopathy, metastasis (spread along gastrocolic ligament causes mets to Transverse colon, spread along gastrohepatic ligament causes liver mets, haematogenous mets to liver, ovaries and adrenals, peritoneal metastases), ascites; Kruckenberg tumour, Virchow’s nodes (mets to left supraclavicular node).
Fig. 7.4.5.4T2WI showing gastric wall thickening with a polypoidal lesion in fundus (arrow) and multiple focal liver lesions in a case of metastatic gastric carcinoma. Source: (Image courtesy Dr Ganesh Saravagi, 167 Military Hospital.)
Lymphoma
Primary gastric lymphomas are usually NHL.
Features suggestive of lymphoma are bulky mass without causing obstruction transpyloric spread, infiltration with preserved fat planes, bulky lymphadenopathy (lymphadenopathy below renal hilum more common than gastric carcinoma), splenomegaly.
May occur as one or more submucosal masses; ulceration and cavitation are common; may appear as Bull’s eye lesions of similar sizes.
Fig. 7.4.5.5Irregular mass-like concentric wall thickening in a case of antral lymphoma. Source: (Image courtesy Dr Amit Bajpai, INHS Asvini.)
Polyps
a) Fundic gland polyps: Associated with use of proton pump inhibitors.
b) Hyperplastic polyps: No malignant potential. Associated with pernicious anaemia.
c) Adenomatous polyps can undergo malignant transformation. Associated with Gardner’s syndrome, Cronkhite–Canada syndrome.
d) Hamartomatous polyps: May be solitary or associated with Peutz–Jeghers syndrome.
Adenomatous – usually solitary, larger (1–4 cm), lobulated or pedunculated, more common in antrum;
Premalignant;
Hyperplastic – usually multiple, small (<1 cm) sessile, occur throughout stomach (more common in body and fundus)
Hamartomatous – multiple occur as clusters.
Small and relatively spare the antrum.
Fig. 7.4.5.6CECT shows rounded well-defined hypodense filling defect seen in fundus due to a gastric polyp. Source: (Image courtesy Brig Giriraj, Dean Command Hospital Chandimandir.)
Metastases
Usually mets to stomach are haematogenous. Rarely lymphatic spread is seen. Stomach can be involved from adjacent organs like oesophagus and kidney.
One or more; most commonly from malignant melanoma or Ca breast; ulceration or cavitation common; may appear as Bull’s eye lesions of various sizes.
Gastrointestinal stromal tumor (GIST)
• Benign to malignant tumours consisting of intersecting bundles of spindle cells in a whorling pattern.
• Earlier they were thought to be a class of heterogeneous smooth muscle tumours ranging from benign leiomyomas to malignant leiomyosarcomas (made of spindle cells) and leiomyoblastomas (made of epithelioid cells).
Now they are thought to arise from interstitial cells of Cajal.
• On immunohistochemistry, they are CD117 (c-kit protein) positive.
GIST grows to a large size before becoming symptomatic (pain/obstruction) because it is located in the submucosa and does not invade locally.
Stomach GISTs are less aggressive.
They may be endogastric, that is, intramural and growing towards the lumen (most common pattern), exogastric or have both endo- and exogastric components.
Rarely multiple; ulceration and fistulous communication with bowel occur in larger tumours; may have hepatic and peritoneal mets (however, lung metastases are rare); ascites and lymphadenopathy are uncommon.
Fig. 7.4.5.7Large lobulated heterogeneously enhancing lesion arising from posterior wall of fundus with a small luminal and large exophytic component. Spleen is inferiorly displaced.
Fig. 7.4.5.8Sagittal section showing the same lesion.
Gastric bezoars
They are composed of concretions of indigestible material which cannot exit the stomach because of their large size and entangled undigested fibres, hair, etc. resulting in gastric outlet obstruction.
Mobile masses; mottled appearance (because of air trapped within the interstitium of the tangled mass) on barium study; free of gastric wall on CT.
Fig. 7.4.5.9Heterogeneous luminal mass separate from gastric wall with trapped air.
7.4.6
APPROACH TO WIDENING OF C LOOP OF DUODENUM
Roma Rai
Clinical history
A 60-year-old male with history of chronic alcohol consumption and chronic weight loss and pain epigastrium presented to Radiology for USG. A finding on USG called for a barium meal and follow-through for academic purpose.
Key findings
Barium meal and follow-through spot image revealed widening of C loop of duodenum along with extrinsic compression on the antrum posteroinferiorly giving rise to classical ‘antrum pad’ sign. There was, however, no obvious mucosal irregularity seen. There is evidence of contrast hold-up.
Analysis and interpretation
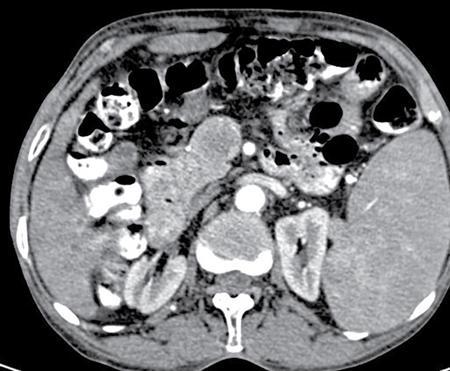
The image showcases two classical signs in GI radiology which are the ‘widening of C loop of duodenum’ and the ‘antral pad sign’. Both the signs are typically described in masses of head of pancreas. A comment on the mucosal lining (regular/irregular) may give a pointer towards the mass being malignant. However, this is a nonspecific sign giving indication of a mass effect and has a variety of differentials. The final diagnosis is reached with the help of cross-sectional imaging and/or endoscopy/biopsy. CECT abdomen in this case confirmed it to be a case of carcinoma pancreas (Fig. 7.4.6.1).
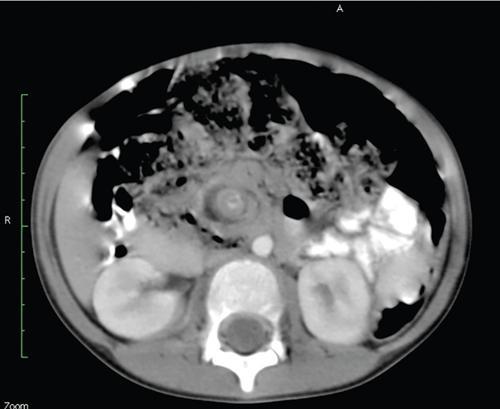
Fig. 7.4.6.1CECT showing a mass in the head of pancreas.
Differential diagnosis
Following are the common and uncommon differential and approach to their diagnosis:
Carcinoma head of pancreas
a) Widening of C loop with irregular mucosal margins.
b) Antral pad sign.
c) Frostberg inverted 3 sign.
d) Definitive diagnosis with CECT.
Fig. 7.4.6.2Barium meal depicting widened C loop of duodenum.
Pseudocyst of pancreas
a) Two classical signs described above.
b) Smooth indentation and smooth mucosa.
c) USG/CT will show the cystic nature.
Fig. 7.4.6.3CECT abdomen showing a large pseudocyst.
Duodenal duplication
a) Unilocular cystic lesion originating in relation to the duodenum. Imaging features may mimic pseudocyst; however, they are usually smaller in size and very rare.
b) Definitive diagnosis using high frequency USG showing classical gut signature.
c) Image on the right shows a case of duodenal duplication cyst along with intestinal malrotation.
Only gold members can continue reading. Log In or Register to continue







 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access