Presentation and Presenting Images
( ▶ Fig. 64.1, ▶ Fig. 64.2, ▶ Fig. 64.3)
A 40-year-old female presents for baseline screening mammography.
64.2 Key Images
64.2.1 Breast Tissue Density
The breasts are heterogeneously dense, which may obscure small masses.
64.2.2 Imaging Findings
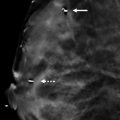
The patient had a conventional digital screening mammogram. There is a possible area of architectural distortion seen posteriorly and superiorly in the left breast around the 12 o’clock location ( ▶ Fig. 64.4 and ▶ Fig. 64.5).
64.3 BI-RADS Classification and Action
Category 0: Mammography: Incomplete. Need additional imaging evaluation and/or prior mammograms for comparison.
64.4 Diagnostic Images
( ▶ Fig. 64.6, ▶ Fig. 64.7, ▶ Fig. 64.8, ▶ Fig. 64.9)
64.4.1 Imaging Findings
As part of the diagnostic imaging, the patient had digital breast tomosynthesis (DBT) of the left breast. Only the DBT images are shown here, and they demonstrate a focal area of architectural distortion ( ▶ Fig. 64.8 and ▶ Fig. 64.9). An ultrasound following the diagnostic imaging did not provide a sonographic correlate to the findings on DBT. The patient was biopsied with stereotactic guidance.
64.5 BI-RADS Classification and Action
Category 4B: Moderate suspicion for malignancy
64.6 Differential Diagnosis
Radial scar: Radial scars when seen mammographically most often present as architectural distortion. DBT is especially effective at identifying architectural distortion.
Carcinoma: Architectural distortion, although less common than other imaging findings, has a high probability of being carcinoma when identified mammographically. This would be considered a concordant diagnosis.
Normal breast tissue: Normal breast tissue does not typically appear as architectural distortion. Even on a baseline mammographic examination, architectural distortion should be completely evaluated and this may require a biopsy.
64.7 Essential Facts
The estimated prevalence of architectural distortion on conventional screening digital mammography is 6%.
ACR BI-RADS Atlas, 5th edition, defines architectural distortion as distortion of the parenchyma with no definite mass visible.
Architectural distortion can be associated with an asymmetry or calcifications.
Architectural distortion is often undetected on conventional digital mammography and is one of the main sources of false-negative mammograms.
64.8 Management and Digital Breast Tomosynthesis Principles
Partyka and colleagues (2014) raised the possibility that areas of architectural distortion seen only on DBT and occult on conventional mammography and ultrasound are more likely to be a radial sclerosing lesion than carcinoma.
DBT is expensive to add into a practice. The expense is not only in the mammography equipment, but also in the storage of large data files and the workstations that are needed to view the image sets.
There is no uniform adoption of DBT into screening or diagnostic mammogram imaging protocols.
64.9 Further Reading
[1] Partyka L, Lourenco AP, Mainiero MB. Detection of mammographically occult architectural distortion on digital breast tomosynthesis screening: initial clinical experience. AJR Am J Roentgenol. 2014; 203(1): 216‐222 PubMed
[2] Shaheen R, Schimmelpenninck CA, Stoddart L, Raymond H, Slanetz PJ. Spectrum of diseases presenting as architectural distortion on mammography: multimodality radiologic imaging with pathologic correlation. Semin Ultrasound CT MR. 2011; 32(4): 351‐362 PubMed

Fig. 64.1 Exaggerated left craniocaudal (XLCC) mammogram.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


