Fig. 2.1
Classification of arthritis
1.
Osteoarthritis
2.
Rheumatoid arthritis
3.
Seronegative arthritis (ankylosing spondylitis, reactive arthritis, psoriatic arthritis, enteropathic arthritis)
4.
Crystalline arthropathies (gout, CPPD)
5.
Connective tissue disorders (SLE/scleroderma/polymyositis/dermatomyositis/Sjogren’s)
6.
Vasculitis
7.
Infectious arthritis
Symptoms
Image interpretation should not be isolated and should be performed in conjunction with available clinical data. One must differentiate the underlying etiology of joint symptoms; the major differentials include inflammatory and mechanical etiologies. Inflammatory conditions typically are worse in the morning with stiffness lasting more than 60 min and improve with movement. Mechanical and degenerative arthritides on the other hand last less than 60 min and are worse with movement. The number and symmetry of joint involvement are helpful in determining the type of arthritis.
Typically arthritis is separated into monoarticular (one joint), oligoarticular (two to four joints), and polyarticular (more than five joints) types (Tables 2.1, 2.2, 2.3, 2.4, and 2.5). That being said, many arthritides can involve any number of joints, but typically fall into one category. Gout and CPPD are inflammatory arthritides that usually start as monoarthritis as does osteoarthritis, but as time passes, other joints can be involved. Psoriatic arthritis (PsA) can have many different presentations including monoarthritis and polyarthritis, which may or not be symmetrical. Rheumatoid arthritis (RA) is the classic inflammatory arthritis with a symmetric polyarthritis that almost always involves the hands. Assessment of synovitis, a process whereby the synovial membrane of a joint is inflamed, is important. It is the mainstay of inflammatory conditions and occurs much more often than in osteoarthritis where it is much less intense and much less widespread.
Table 2.1
Differential diagnosis of common causes of acute monoarthritis
Infectious (bacterial, viral) |
Crystalline |
Traumatic |
Seronegative spondyloarthropathy (PsA, reactive) |
Hemarthrosis |
Table 2.2
Differential diagnosis of common causes of chronic monoarthritis
Infectious (TB, fungal, Lyme) |
Seronegative arthritis (reactive, AS, PsA, enteropathic) |
Noninflammatory (OA, AVN) |
Pigmented villonodular synovitis |
Foreign body synovitis |
Table 2.3
Differential diagnosis of common causes of oligoarthritis
Infectious (bacterial endocarditis, nongonococcal, disseminated GC, viral) |
Postinfectious (reactive, poststreptococcal) |
Seronegative arthritis (reactive, AS, PsA, enteropathic) |
Oligoarticular presentation of atypical inflammatory arthritis (RA, SLE, adult onset Still’s) |
Table 2.4
Differential diagnosis of common causes of acute polyarthritis
Infectious (viral) |
Rheumatoid arthritis |
Systemic lupus erythematosus |
Early disseminated Lyme |
HIV |
Bacterial endocarditis |
Psoriatic arthritis |
Polyarticular gout |
Table 2.5
Differential diagnosis of common causes of chronic polyarthritis
Rheumatoid arthritis |
SLE |
Psoriatic arthritis |
Other connective tissue disorders |
Polyarticular gout |
CPPD (pseudo-RA) |
Sarcoid arthritis |
Vasculitis |
Sarcoid arthropathy |
The onset of clinical symptoms can be helpful when trying to narrow down the diagnosis to a particular disease. RA is typically subacute occurring over weeks to months rather than days. Osteoarthritis is of gradual onset, usually over many years with slow progression. Crystalline arthropathies, such as chronic CPP arthritis, can also present like osteoarthritis. Septic arthritis and acute crystalline arthritis can present acutely with rapid progression of symptoms in a matter of hours.
Weakness is another symptom that is important to further clarify. This may be subjective as in patients with polymyalgia rheumatica, where the stiffness can be so great as to cause a feeling of weakness, and when questioned, some patients state that it affected them so greatly that they had to crawl to get out of bed. However, when tested objectively, no weakness is found. This subjective stiffness and pain is symmetric and proximal. In the case of polymyositis, however, the patient has very little stiffness but is both subjectively and objectively weak when tested in the proximal musculature (shoulder and hip girdle). Weakness may alternatively be neuropathic in nature, is more often distal in nature, and is associated with other neurological symptoms.
Family history becomes particularly important when looking at the group of disorders called the seronegative spondyloarthropathies (seronegative arthritis) as they occur much more commonly in HLA-B27-positive families as well as the associated disorders of inflammatory bowel disease.
Axial Versus Peripheral Involvement
Peripheral involvement can include specific patterns like distal and proximal interphalangeal involvement (DIP/PIP) in osteoarthritis and psoriatic arthritis or proximal interphalangeal and metacarpophalangeal joint (PIP/MCP) involvement in rheumatoid arthritis, psoriatic arthritis, SLE, and pseudo-RA (crystalline arthropathy of calcium pyrophosphate dihydrate or CPPD). Acute involvement of one joint that is red, hot, and swollen should trigger one to think of a septic arthritis, gout, or pseudogout.
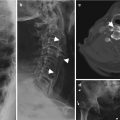
Axial involvement can help narrow the type of arthritis down as well. Lower back involvement is not a characteristic of rheumatoid arthritis, gout, SLE, or systemic vasculitis but is mandatory in that of ankylosing spondylitis. Peripheral involvement with axial involvement could mean osteoarthritis, ankylosing spondylitis, psoriatic arthritis, or reactive arthritis. Involvement of the cervical spine is frequent in rheumatoid arthritis as well as osteoarthritis.
Other Features
Systemic features can often point to a more definitive rheumatic etiology and these features should actively be sought after. Constitutional features of fever, anorexia, weight loss, and fatigue are more associated with an inflammatory process. Nonarticular features such as a history of bloody diarrhea or a genitourinary infection can be highly associated with an inflammatory bowel disease and enteropathic arthritis or that of a reactive arthritis respectively. Specific symptoms of dry eyes (xerophthalmia) and dry mouth (xerostomia), Raynaud’s, and specific rashes such as malar, discoid (systemic lupus erythematosus), Gottron papules, shawl sign, V-neck sign, mechanic’s hands, and heliotrope rash (dermatomyositis) can help clinch the diagnosis of a connective tissue disorder. Digital ulcers, puffy fingers, and Raynaud’s are all highly suggestive if not diagnostic of systemic sclerosis (scleroderma).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


