Bariatric Surgery
Michael P. Federle, MD, FACR
Key Facts
Imaging
Laparoscopic adjustable gastric banding (LAGB) procedure (a.k.a. “lap band”)
Complications: Less common and less varied
May be too tight or too loose
May erode into stomach or esophagus
→ leak of contrast material on UGI or CT
Laparoscopic Roux-en-Y gastric bypass procedure; bariatric procedure of choice in North America
Gastrointestinal complications occur in about 10%
Anastomotic leaks
Most commonly at gastrojejunal anastomosis
CT may demonstrate major and minor leaks; fluid collections not evident on UGI series
Small bowel obstruction (SBO)
Most common etiology: Internal hernias (IH) and adhesions
IH: CT appearance depends on location
Clustering of SB loops; congestion, crowding, twisting of mesenteric vessels
Anastomotic stricture
Dilatation of gastric pouch; spherical shape; air-fluid-contrast material levels
Usually responds to balloon dilation
Obstruction and perforation of distal stomach
Cannot be diagnosed with UGI series; CT is key
May progress to perforation (often fatal)
Marginal ulcers; rate of 0.5-1.4% after RYGB
Usually result of ischemia
CT and UGI radiography; complementary roles
Top Differential Diagnoses
Ileus
Reflux into excluded stomach
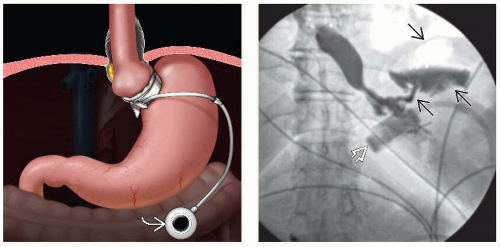 (Left) Graphic depicts the gastric banding procedure in which a silicone band is looped around the proximal stomach. A tube connects the inflatable liner of the band to a subcutaneously placed port  that can be accessed and inflated or deflated with injections of fluid. (Right) Upper GI series shows a leak that can be accessed and inflated or deflated with injections of fluid. (Right) Upper GI series shows a leak  of gas and contrast medium following placement of a gastric band of gas and contrast medium following placement of a gastric band  around the gastric fundus. around the gastric fundus. |
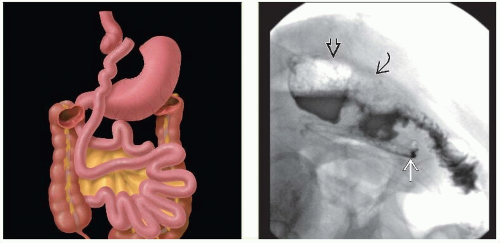 (Left) Graphic shows the typical procedure for a Rouxen-Y gastric bypass procedure, with a small gastric pouch anastomosed to a Roux limb that is 75-150 cm long, and which is anastomosed side-to-side with the “biliopancreatic” limb about 35-45 cm beyond the ligament of Treitz. (Right) RYGB procedure. Upper GI series shows minor anastomotic leak, evident only as opacification of the surgical drain  that was placed near the gastric pouch that was placed near the gastric pouch  ; the “pouch-enteric” anastomosis is noted ; the “pouch-enteric” anastomosis is noted  . . |
TERMINOLOGY
Definitions
Complications of surgical procedures meant to induce weight loss
IMAGING
General Features
Morphology
Laparoscopic adjustable gastric banding (LAGB) procedure (a.k.a. “lap band”)
Silicone band with inflatable cuff is looped around fundus, about 3 cm below GE junction
Opening (stoma) is adjustable by accessing subcutaneous port connected to inflatable cuff
Fluid is injected into or removed from port to inflate or deflate cuff
Complications: Less common and less varied than in laparoscopic Roux-en-Y gastric bypass (RYGB) procedure
Twisting or displacement of band
Should lie at an angle; cephalic side at about 1-2 o’clock position; caudal at about 7-8 o’clock
May slip down, leaving excessively large pouch, or slip up, leaving excessively small pouch
May be too tight (→ nausea, dehydration, excessive weight loss) or too loose (→ insufficient restriction of food intake)
May erode into stomach or esophagus
Leads to leak of contrast material on UGI or CT
Laparoscopic Roux-en-Y gastric bypass procedure; bariatric procedure of choice in North America
RYGB procedure
Gastric pouch: 15-30 mL; excluded from distal stomach
Anastomosed end to side to Roux-en-Y limb
Distal gastric remnant (excluded stomach) left in its normal anatomic position
Roux-en-Y limb; created by transection of jejunum at 35-45 cm distal to ligament of Treitz
Roux limb is 75-150 cm long
Anastomosed side-to-side with proximal jejunum
Roux limb may be brought through transverse mesocolon to be placed in retrocolic position
Or anterior to transverse colon (and stomach)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


