1 Over the past few decades, the use of ultrasound in ophthalmology has become an important and often necessary tool to aid in the diagnosis of intraocular and orbital disease. It is employed most frequently when ophthalmoscopic evaluation is limited or when differentiation of mass lesions or other pathology is needed. Imaging of the eye and orbit is facilitated by the use of high frequency sound (8–10 MHz, 20 MHz, and 50–100 MHz). The sound wave is transmitted and received through a probe that is placed directly on the eye or on the eyelid. As sound travels through the structures of the eye, reflected signals are returned to the probe, mechanical energy is converted to electrical energy, and signals or echoes are recorded on an oscilloscope. The techniques of standardized echography and the descriptions of typical echographic features of selected disorders are described in this second edition atlas. The term standardized echography was first used by Dr. Karl Ossoinig, and refers to the combined use of a contact B-scan (brightness modulation) and a standardized A-scan (amplitude modulation) to evaluate ocular and orbital pathology using prescribed examination techniques. Dr. Ossoinig is credited with the development of the first standardized A-scan. The A-scan provides a one-dimensional image of spikes or deflections of varying amplitude along a baseline. Because of the amplification design of this equipment, differentiation of tissue is possible based on the reflectivity (height of spikes) and structure (distribution of spikes) produced by the cells of various tissue. Sound attenuation, consistency, vascularity, and precise measurements are also determined with the A-scan. The B-scan, on the other hand, allows for two-dimensional imaging of a series of dots and lines that form the echogram. B-scan imaging is most useful for determining the topographic features of the normal globe structures as well as abnormal structures that may be present. A simplified way of describing the need for both contact B-scan and standardized A-scan imaging is to compare the B-scan with color fundus photography and the A-scan with fluorescein angiography. The B-scan or fundus photograph may provide some useful information, but it may not be enough to confirm a diagnosis. Adding standardized A-scan or fluorescein angiography to the evaluation may provide additional information necessary to make a differential diagnosis. Thorough echographic examination of the eye is critical to obtain accurate, reproducible results. Adhering to a methodical screening pattern will ensure that all segments of the globe have been examined and will help the echographer feel more confident about which probe position correlates with the area of the eye being examined at any given time. The location of the equipment in the room and a reclining chair in close proximity to the machine are important considerations prior to beginning an ultrasound examination. The patient’s head should be positioned close to the screen, and the echographer should be comfortably seated within easy reach of the buttons and knobs. After explaining the procedure to the patient, an anesthetic drop should be administered to each eye. Even if the examination is only requested for one eye, it is helpful to numb both eyes in case comparison from one to the other is warranted. Having a fixation device that the patient can follow is also recommended. It is best to perform the examination with the probe placed directly on the globe. Doing so allows the echographer to control the patient’s gaze and it also decreases the amount of sound attenuation that occurs when the probe is placed on the lids. A coupling agent such as methylcellulose is needed to facilitate sound transmission and to minimize the amount of air that can be trapped between the probe surface and the globe. Key vocabulary used to describe contact B-scan probe positions includes; probe marker perpendicular, parallel, axial, and oblique sound beam orientations. The B-scan probe has a single piezoelectric crystal that moves back and forth toward the marker located on the external portion of the probe. This marker may be a small dot or a single line, depending on the equipment manufacturer. The orientation of the marker is directly correlated to the sound beam orientation. Wherever the marker is directed on the eye represents the upper portion of the echogram and, in most instances, the probe is placed opposite the area of the eye to be examined. To simplify the screening sequence, the probe should be held with the marker either directed toward the nose or in an upright position toward 12 o’clock. To evaluate the superior or inferior fundus, the marker should be directed toward the nose so that the sound beam is moving horizontally (horizontal transverse). Conversely, to evaluate the nasal or temporal fundus, the marker should be directed toward the 12-o’clock meridian so that the sound beam is moving vertically (vertical transverse). Because the center of the sound beam offers the best resolution and detail, if significant pathology is located superonasally, inferonasally, superotemporally, or inferotemporally, the probe position and marker placement should be adjusted to display the pathology in the center of the echogram (oblique transverse). In these instances, the marker should be directed toward one of the upper meridians of the globe. When the globe is evaluated using vertical, horizontal, or oblique transverse probe positions, the sound beam is aimed perpendicular to the globe wall and only a 2-mm slice of tissue along 6 clock hours is being evaluated. Therefore, it is essential to shift the probe from the corneal limbus to the fornix to view all areas of the globe adequately. Failure to do so may lead to either misdiagnosis or missed diagnosis of intraocular findings. The most useful examination sequence using transverse scans is to first evaluate the superior, then nasal, inferior, and temporal fundus, respectively. Once all four quadrants of the eye have been examined using the transverse or cross-sectional views, it is suggested that the eye then be evaluated using longitudinal (radial) probe positions. For these, the sound beam is aligned parallel to the fundus, and the image produced is of a single clock hour from the posterior pole to the periphery. To achieve this, the marker again becomes an important feature of orientation. It can be directed anywhere along the corneal limbus, opposite the area of the eye to be evaluated. Using both transverse and longitudinal probe positions enables the echographer to build a three dimensional picture of the intraocular structures. An additional B-scan probe position that can be utilized and often provides additional topographic features of abnormal structures is the axial (anteroposterior) scan. A thick layer of methylcellulose should be used, and the probe is placed gently on the cornea. With the probe in this position, the echographer can evaluate a thin section of tissue from the front of the eye to the back of the eye. Because there may be significant sound attenuation (absorption) from the lens, the axial scan may not be the most optimal probe position to use; however, it is an excellent method to evaluate pathology and its relationship to the lens and optic nerve.
Basic Screening Techniques and Indications for Ultrasound
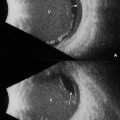
 Contact B-Scan
Contact B-Scan
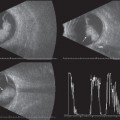
 Standardized A-Scan
Standardized A-Scan
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


