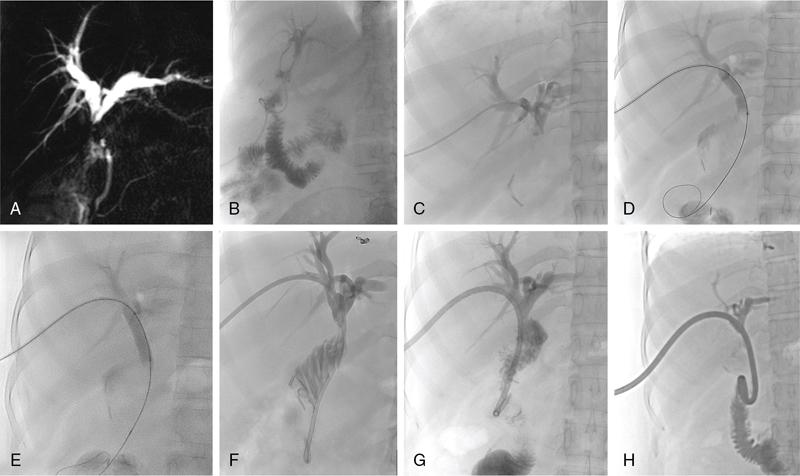
The aetiologies for BBS include iatrogenic, autoimmune, infectious, inflammatory and congenital causes. The most common cause is an iatrogenic stricture developing after cholecystectomy (0.5%–0.7% of cholecystectomies), liver transplantation (10%–40% of liver transplantation surgeries) and pancreatobiliary surgeries. Treatment varies based on the aetiology and the type of stricture. Differentiation of benign and malignant stricture is essential prior to percutaneous intervention. The diagnosis of BBSs should be made carefully by a combination of clinical history, cross-sectional imaging studies and surgical details. These patients can be asymptomatic presenting with altered laboratory parameters or have clinical symptoms such as anorexia, jaundice, fever with chills due to cholangitis and abdominal pain. In chronic cases, patients may also develop secondary biliary cirrhosis and subsequently liver failure. Bile leaks are associated mostly with cholecystectomy, hepatectomy and pancreatobiliary surgeries. Bile leak results in biliary peritonitis, biloma, abscess and increases the risk of septicemia. Although, surgery is the mainstay for the management of BBSs, the role of endoscopy-guided management is now considered equally safe and effective. Percutaneous management is indicated in patients who are poor surgical candidates or those with failed or difficult endoscopic access due to unsuccessful cannulation or altered anatomy such as in a Roux-en-Y hepaticojejunostomy or a distal gastrectomy. The aim is to relieve the obstruction and then either to prepare the patient for surgery or to perform additional percutaneous interventions. In patients with bile leak, PTBD causes diversion of bile and thus allows healing of the site of leak. The most common indication is postoperative bile leak. The first step is to confirm the benign nature of the stricture. Review of clinical history, clinical examination and lab parameters is of paramount importance. History of cholecystectomy, liver transplantation or a pancreatobiliary surgery provides clues towards a benign stricture. Imaging helps in noninvasive assessment. USG, contrast-enhanced CT and MRI with MRCP are all useful and may help to characterize the stricture. A plan is to be formulated based on the imaging findings. Often bile leak is confirmed by the persistent drainage of bile in the drainage catheter. Imaging in such cases may not be needed. However, more frequently, MRI with MRCP is performed to define the anatomy of the bile ducts, anatomical variations and possible site of bile duct injury and leak. This will help plan the percutaneous interventions. Presence of ascites, biloma and liver abscesses require additional drainage. Reviewing the blood laboratory parameters and obtaining informed consent, are similar to other intervention procedures. Up to 30% of patients with non-malignant biliary strictures may have a protracted, complicated course requiring multidisciplinary management. In patients where other procedures are not suitable, percutaneous methods may be utilized. The techniques available include balloon dilatation of the stricture, percutaneous large calibre drain placement or stent placement. The steps for PTBD are the same as described previously. Benign strictures usually produce less upstream dilatation and thus 21G or 22G needle is required for the initial duct puncture. It may be difficult to internalize the drainage catheter due to dense fibrosis at the site of the stricture. In such cases an external drainage catheter should be left in situ and internalization may be re-attempted after 2–3 weeks. Few additional percutaneous procedures are performed to open these strictures as repeat surgery or endoscopic approach is difficult. Short-segment unifocal strictures respond better to balloon dilatation with short-term patency ranging from 50% to 90% and long-term patency of 56%–74%. Strictures developing in the early postop period (<1 month) after liver transplantation may be secondary to oedema or kinking of the duct and these also do not respond well to balloon dilatation. The procedure involves crossing the stricture with a guidewire, followed by balloon dilatation (Fig. 9.24.15). The diameter of the balloon chosen should be at least as large as the bile ducts proximal and distal to the obstruction and may be oversized by up to 20%–25%. Further oversizing may cause rupture leading to bleeding or bile leak. Following dilatation, a drainage catheter is usually left in situ to allow healing around the catheter. The dilatation process may be repeated at 4-week intervals to improve patency.
7. Benign biliary strictures and bile leaks
Indications for drainage
Preprocedure evaluation
BBSs
Bile leak
Methods of treatment of BBSs
PTBD for drainage
Balloon dilatation
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


