Inflammatory bowel disease (IBD) has a rising prevalence in children and an increasing number of adults living with IBD were diagnosed in childhood. This chronic disorder requires frequent cross-sectional imaging for evaluating disease progression. Radiologists must be vigilant to detect and understand imaging manifestations of acute and chronic, alimentary, and extraintestinal findings of IBD. This article discusses the role of imaging in evaluation of IBD transitioning from pediatric to adult patients. Imaging modalities and techniques used for evaluating IBD are reviewed. Characteristic acute and chronic imaging findings of IBD are discussed with emphasis on what radiologists need to clearly understand.
Key points
- •
Inflammatory bowel disease (IBD) prevalence continues to rise in children and now there is an increased number of adults living with IBD diagnosed in their childhood.
- •
IBD presents differently in children compared with adults, with more aggressive, multisegmental disease. Small bowel obstruction is less common than in adults.
- •
As pediatric patients transition to the adult population, they begin to experience similar complications and phenotype of those who present in adulthood.
- •
Magnetic resonance enterography (MRE) remains the reference standard for evaluating patients with IBD, although there is a role for other imaging modalities, which should always be considered, depending on clinical presentation.
- •
Differentiating fibrotic from inflammatory disease is a shortcoming in current IBD imaging and an area of research.
Introduction
Inflammatory bowel disease (IBD) has become more prevalent in recent years. Although the disease is classically divided into Crohn disease (CD) and ulcerative colitis (UC), patients may also be diagnosed with unclassified IBD in the pediatric population. In the United States, the prevalence of UC in adults reaches 238 per 100,000 and 201 cases of CD per 100,000. Among adults, younger patients (ages 20–29) have a higher prevalence of CD. Some of the increasing prevalence of IBD in recent years is on account of improving life expectancy. An added contributor, however, is the diagnosis of childhood IBD; up to 20% of patients with CD and 12% of patients with UC are diagnosed younger than 20 years old. Therefore, there is now an increased number of adults living with IBD diagnosed in their childhood.
This review article discusses the role of imaging in evaluation of IBD transitioning from pediatric to adult patients. Imaging modalities and techniques currently used for evaluating IBD are reviewed. In addition, the spectrum of characteristic acute and chronic imaging findings of IBD is discussed with emphasis on what general radiologists need to clearly understand.
Role of imaging in evaluation of inflammatory bowel disease: transitioning from pediatric to adult patients
Adolescents diagnosed with IBD tend to present differently from adult patients, and this should be considered when performing imaging studies. CD is more likely to be ileocolonic, rather than confined to small bowel. Gastric involvement, although less common, is typically a feature of pediatric rather than adult disease. UC is more likely to diffusely involve the colon rather than segments of it. Stricture and obstruction are more common in adults, but as IBD progresses, the risk for these complications increases in children. Children and adults exhibit extraintestinal manifestations at similar rates, and one should always be mindful to look for these complications on imaging studies.
Imaging techniques
Until recently, there had been a lack of consensus as to the imaging modality of choice for evaluation and surveillance of IBD ( Table 1 ). However, as technique for magnetic resonance enterography (MRE) has advanced, it has emerged as the preferred method of serial imaging pediatric patients with IBD. , Still, a meta-analysis of more than 14,000 patients revealed that all modalities have comparable detection rates of IBD in children ; for this reason, ultrasound remains an alternative to MRE for imaging of IBD.
| Modality | Advantages | Disadvantages | Essential Techniques |
|---|---|---|---|
| Radiography | Easily accessible Can identify surgical emergency (ie, perforation) | Neither sensitive nor specific | Supine and upright anteroposterior abdominal radiography |
| Ultrasound | Low cost No radiation No sedation No gadolinium Good spatial resolution Good if MRE not available | Operator dependent Limited evaluation of sigmoid colon and rectum Limited evaluation of extraintestinal disease | Longitudinal and transverse representative images in all four quadrants with and without color Doppler High-frequency linear transducer |
| Computed tomography | Widely available No sedation Good spatial resolution | Ionizing radiation | Intravenous and enteric contrast Axial and coronal multiplanar reformats Neutral enteric contrast to opacify the small bowel is preferred |
| Magnetic resonance imaging | No ionizing radiation Excellent contrast resolution Good anatomic detail on SSFP images | Vulnerable to respiratory and susceptibility artifact Gadolinium required Spasmolytics required Sedation may be needed | SSFSE axial SSFSE coronal with cine loop Axial and coronal T2-weighted fat-suppressed Coronal T1-weighted fast-suppressed postgadolinium in 3 dynamic phases, including early mesenteric phase Diffusion weighted imaging preferred Dedicated small field of view if perineal fistula a concern |
Radiography
When evaluating IBD, radiography serves as an entry point for clinical investigation, rather than a sole method for achieving diagnosis. Children with new-onset IBD may present with ongoing abdominal pain, for which an abdominal radiograph is often requested. Typically, images are obtained with patients in the upright and supine position.
Ultrasound
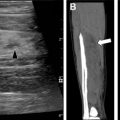
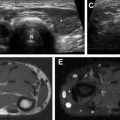
Individual protocols for evaluation of the gastrointestinal tract may vary by institution. However, to optimize the excellent spatial resolution of ultrasound, it is important to evaluate the small and large bowel with a linear high-frequency transducer. Such high-frequency transducer can demonstrate intestinal segments in longitudinal and transverse axes. Color Doppler imaging can further evaluate abnormal findings, such as hyperemia in the setting of active inflammation. Unfortunately, because of the limited acoustic window, adequate sonographic interrogation of the sigmoid colon and rectum is often more difficult.
Computed Tomography
Abdominal computed tomography (CT) provides excellent spatial resolution, and rapid imaging capability obviates breath-holding. Spasmolytic agents, an essential component of MRE, are not necessary with CT. An obvious disadvantage is the use of ionizing radiation. Patients with IBD require multiple studies over time, further rendering this modality suboptimal in a younger population. When evaluating IBD, it is best to opacify the small bowel with a neutral oral contrast agent. Intravenous contrast should be administered to increase the conspicuity of inflammation.
Magnetic Resonance Imaging
Magnetic resonance (MR), specifically MRE, with excellent contrast resolution, has become the cornerstone of imaging children and adolescents with IBD ( Table 2 ). The field of view extends from the lung bases through the perineum, with additional smaller field-of-view imaging of the perineum if there is concern for perianal fistula. Flexible phased-array body coils, and the built-in spine coil, are used. Imaging may be performed on either a 1.5- or 3.0-T strength magnet. The 3.0-T magnet allows for superior spatial resolution, signal, and contrast-to-noise ratio. There is, however, greater susceptibility artifact secondary to intra-abdominal gas and surgical material. Fat suppression is difficult on 3.0-T magnets, necessitating acquisition of images in two stacks (upper and lower) with separate shim boxes to reduce inhomogeneity.
| Exam | Indication | Full Protocol | Additional Elements |
|---|---|---|---|
| MRE | Assessment of small intestine involvement (primary) Assessment of colon (secondary) Assessment of extraintestinal manifestations (secondary) Assessment of intra-abdominal fistula | Body matrix coil Axial SSFSE Coronal T2-weighted fat-suppressed Axial T2-weighted fat-suppressed Coronal SSFSE with cine loop for peristalsis Axial diffusion weighted imaging Multiphase dynamic coronal VIBE postgadolinium Axial VIBE postgadolinium | Gadolinium (0.1 mL/kg) Glucagon Polyethylene glycol Examination time: 45 min |
| MR imaging pelvis | Assessment for perirectal abscess (primary) Assessment of perianal fistula (primary) Assessment of small intestine involvement (secondary, if low-lying terminal ileum) Assessment of extraintestinal manifestations (secondary, sacroiliac joints) | Body matrix coil Sagittal FSEIR Oblique axial SSFSE Oblique axial T2-weighted fat-suppressed Oblique coronal FSEIR Oblique coronal T1-weighted Oblique axial T1-weighted fat-suppressed postgadolinium Oblique coronal T1-weighted fat-suppressed postgadolinium Sagittal T1-weighted fat-suppressed postgadolinium) | Small field of view Gadolinium (0.1 mL/kg) Examination time: 78 min |
Fluid-sensitive sequences are rapidly acquired in the axial and coronal planes. Single-shot fast spin echo and balanced steady-state free-precession sequences optimize anatomic evaluation. Fat-suppressed MR images increase the conspicuity of inflammation. Diffusion weighted imaging, although bereft of spatial resolution, has excellent sensitivity for detection of inflammation and lymphadenopathy. Single-shot fast spin echo in the coronal plane is used to acquire cine MR imaging sequences to evaluate peristalsis. Postcontrast MR imaging is performed dynamically, first in the mesenteric phase (45–55 seconds postinjection), followed by two successive acquisitions to evaluate bowel wall enhancement over time. To decrease respiratory motion artifact, breath-hold imaging is performed.
Intrinsically T1 hypointense oral contrast is given to distend the small bowel, which improves the ability to detect mucosal and bowel wall disease. The media must be hyperosmolar to optimize terminal ileal distention. To reduce motion artifact caused by bowel peristalsis, paralytic agents, such as glucagon, are administered before contrast injection. , Pediatric patients may have difficulty with breath-holding instructions, and respiratory triggered or radial noncartesian acquisitions may be performed.
Spectrum of imaging findings
Acute Findings of Inflammatory Bowel Disease
In the acute setting, IBD typically manifests with bowel wall inflammation. Radiography may reveal layering fluid within segments of bowel. If there is colonic disease, edema within the bowel wall causes the thickened haustra to project into the aerated lumen (thumbprinting sign) ( Fig. 1 ). In most instances, however, cross-sectional imaging is requested for further evaluation, irrespective of the radiograph findings. In more advanced cases, additional findings include peri-intestinal fat induration, and engorgement of the adjacent vasa recta ( Fig. 2 ). MRE can aid clinicians in distinguishing disease amenable to medical therapy from that requiring surgical intervention. Bowel wall thickening greater than 3 mm, intramural T2 prolongation, and restricted diffusivity are sensitive for active disease requiring a pharmacologic regimen ( Fig. 3 ). , Segmental arterial phase hyperenhancing bowel may also indicate active IBD ( Fig. 4 ).

Related posts:
 Brain Malformations at All Ages
Brain Malformations at All Ages
 Repaired Congenital Heart Disease in Older Children and Adults
Repaired Congenital Heart Disease in Older Children and Adults
 Interstitial Lung Diseases in Children, Adolescents, and Young Adults
Interstitial Lung Diseases in Children, Adolescents, and Young Adults
 Cystic Fibrosis from Childhood to Adulthood
Cystic Fibrosis from Childhood to Adulthood
 Spectrum of Imaging Manifestations of Vascular Malformations and Tumors Beyond Childhood
Spectrum of Imaging Manifestations of Vascular Malformations and Tumors Beyond Childhood
 Congenital Incidental Findings in Children that Can Be Mistaken as True Pathologies in Adults
Congenital Incidental Findings in Children that Can Be Mistaken as True Pathologies in Adults
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


