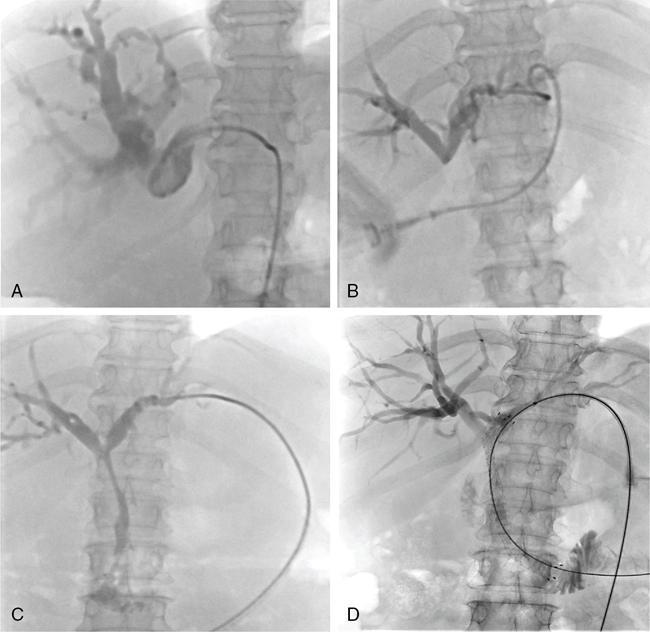
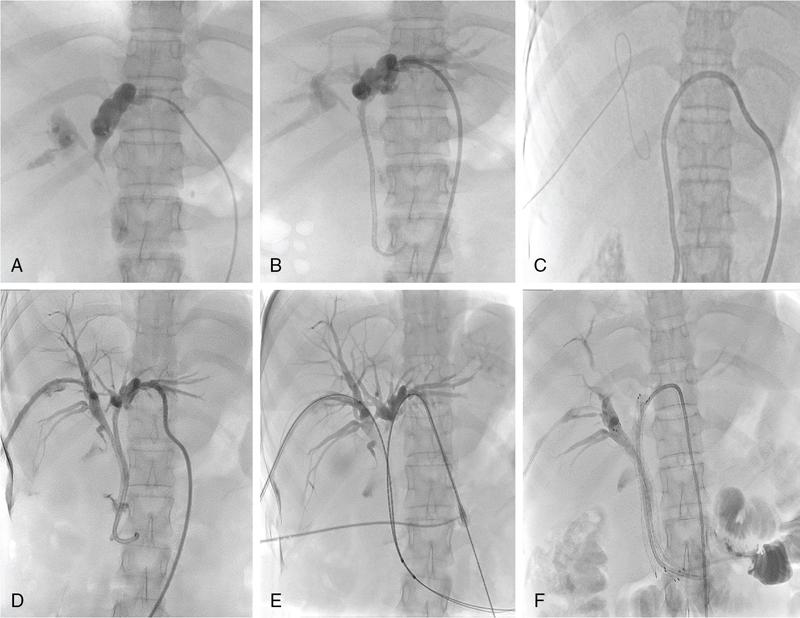
In patients with unresectable malignant biliary obstruction, biliary drainage provides palliation. External or combined internal–external drainage PTBD catheter is uncomfortable for the patient, requires constant care and causes psychological discomfort. Catheter-related complications such as pericatheter leak, tube blockage and kinking and dislodgement occur frequently and add to the morbidity of the patient. Placement of a stent for internal drainage overcomes these complications. Indications for metallic stents include malignant biliary obstruction, mostly in nonresectable cases. Uncommonly, retrievable stents are also placed for BBSs. Stents may be placed intrahepatically for tumours beyond hilum (unilateral or bilateral), in the bile duct and even as bowel stents where tumours invade the gastrointestinal tract beyond ductal entry. There are no absolute contraindications for biliary stenting. Relative contraindications are similar to that for PTBD. Preprocedure imaging is important to identify the type and location of the malignancy. This often helps to decide whether unilobar (Fig. 9.24.12) or bilobar stent (Fig. 9.24.13) is needed. It also helps to define the length of the stricture, although, length of the stent is based on cholangiographic measurements. Further, imaging is important to confirm that the disease is unresectable, as placement of stent makes surgery challenging in resectable cases. Patient preparation is similar to that for PTBD. The initial steps are same as for PTBD till the point of internalization. Then, either the stent is placed as a primary procedure or later as a secondary procedure. After placement of a stiff guidewire, the stent device is inserted over it. The ideal position of the stent is when its proximal and distal ends extend at least 1 cm and preferably 2 cm from the proximal and distal ends of the stricture, respectively. After stenting, an access catheter (5F) is usually placed in situ and the stent is evaluated with a cholangiogram after 48 hours. The metallic stent self-expands and allows internal biliary drainage with resultant decompression of the biliary system. The self-expanding metal stents are made of nitinol, and have thermal memory, allowing them to expand to their maximum diameter when they reach body temperature. This usually occurs in 24–48 hours. In cases, where the stent fails to expand adequately even after 48 hours, percutaneous balloon dilatation of the stent through the access catheter should be done for successful drainage. There are two broad categories of stents: plastic and metallic. Metallic stents can further be divided as covered and uncovered. Plastic stents are placed endoscopically and generally used for benign strictures. They have lower patency rates, require longer hospital stay and a higher overall cost, making them less suitable as palliative stents. Stent-related complications are being increasingly recognized due to the increased life expectancy of patients with stent insertions. This is attributed to the improved palliative care and management of these patients. The complications can be divided into early and delayed (Table 9.24.4).
2. Biliary stenting
Indications/contraindications
Contraindications
Preprocedure evaluation and patient preparation
Procedure details
Complications and management
Radiology Key
Fastest Radiology Insight Engine