The urinary bladder is a part of the lower urinary tract. It is an extraperitoneal structure situated in pelvis and functions predominantly as a reservoir of urine.
A variety of pathological conditions may involve the urinary bladder, which can be congenital, traumatic, infective, inflammatory and neoplastic. Most of these conditions manifest with dysuria, difficulty in micturition or haematuria. On imaging, few of these pathologies can show specific signs. But most of the lesions either present with focal or diffuse thickening of urinary bladder wall creating a diagnostic dilemma. Cystoscopy and histopathological examination in these cases help in coming to a final diagnosis. Imaging in such instances helps in assessing multiplicity of lesions, extravesical spread, the affliction of other organs and associated complications if any.
Imaging modalities to assess the urinary bladder include radiography, ultrasonography, micturating cystourethrography, intravenous urography, CT and MR Urography. While USG remains the initial modality of choice, CT and MR because of their multiplanar capability are the preferred imaging modality in most of the cases, with MR providing superior soft-tissue contrast. However, conventional procedures like micturating cystourethrography and intravenous urography still have a role to play in diagnosis, particularly in patients with obstructive uropathy.
Urachal pathologies
The urachus or the median umbilical ligament is developmentally the obliterated remnants of the allantois and the cloaca. It extends from the dome of the urinary bladder to the umbilicus in the midline (Fig. 10.13.1). It lies in the retropubic space of Retzius in between the transverse fascia and the parietal peritoneum and is extraperitoneal in location.
Fig. 10.13.1Sagittal CT image showing the normal median umbilical ligament-obliterated urachus (white arrow).
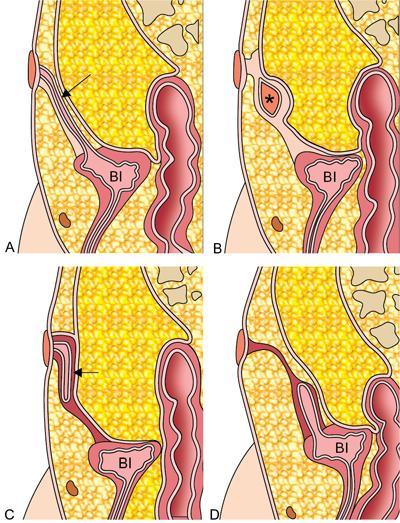
Failure of the urachus to obliterate may lead to four types of congenital Urachal anomalies (Graphic 10.13.1) which include:
1. Patent Urachus (most common, 47%)
2. Urachal cyst (30%)
3. Urachal sinus (18%)
4. Vesicourachal diverticulum (3%)
Graphic 10.13.1Pictorial illustration of urachal anomalies – patent urachus (black arrow in A), urachal cyst (asterisk in B), urachal sinus (black arrowhead in C) and vesicourachal diverticulum (white arrowhead in D) (Bl – bladder).
Recent literature, however, suggests that the urachal cysts may be the most common urachal anomalies (69%).
Urachal anomalies may remain asymptomatic and are sometimes incidentally detected. However, in a few cases, these are diagnosed when they presented with umbilical discharge, super-added infection, calculus formation or rarely when they develop neoplasms.
Ultrasound remains the initial imaging investigations. Sinogram, Micturating cystourethrogram, CT and MRI are also helpful in diagnosing these anomalies and in evaluating for associated complications.
Patent urachus
In this entity, the entire urachus remains patient, resulting in urinary leakage from the umbilicus. It is also known as a urachal fistula.
It is generally diagnosed in the neonatal period when a persistent discharge from umbilicus, oedema around the umbilicus or delayed healing of the umbilical cord stump raises clinical suspicion.
Ultrasound reveals tubular structure in midline extending from bladder dome to the umbilicus, containing anechoic fluid and with echogenic walls. Sinogram and micturating cystourethrogram show contrast-filled tubular tract between the umbilicus and the urinary bladder. Additionally, micturating cystourethrogram helps in ruling out vesicoureteric reflux which is believed to be associated with the patent urachus. CT or MR may be required if there is any doubt in diagnosis or to rule out complications.
Urachal cyst
The urachal cyst is formed when the superior and inferior ends of the urachus are obliterated, leaving behind a fluid-filled cystic structure. It generally involves the lower one-third of the urachus. Most of the times, the urachal cyst is incidentally diagnosed; however, imaging is warranted when there is any complication.
Ultrasound reveals a well-defined cystic structure along the expected course of the urachus in the midline. CT and MR though not needed, may diagnose the cyst incidentally.
Urachal sinus is formed when the umbilical end of the urachus fails to obliterate, resulting in a blind outpouching of the urachus underneath the umbilicus. It is a potential space wherein cellular debris accumulates, and super-added infection may occur. Fluid stasis may also result in stone formation.
Patient presents with intermittent discharge from the umbilicus.
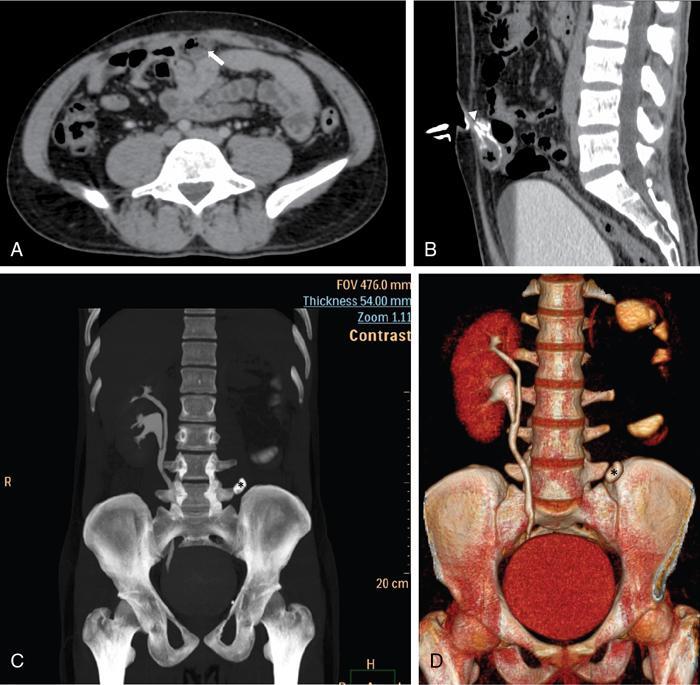
Fig. 10.13.2CECT axial image (A) of a patient who presented with recurrent foul-smelling discharge from umbilicus showing peripherally enhancing collection (white arrow) with air foci at the level of umbilicus in midline. CT sinogram sagittal image (B) revealed contrast lined tract (white arrowhead) communicating the collection with the external sinus confirming the diagnosis of urachal sinus with abscess formation. MIP coronal (C) and volume-rendered image (D) showing the same patient also having an incomplete duplex renal moiety on right side with ureteric calculus (asterisk) on left side.
A sinogram study helps to rule out any communication with the urinary bladder.
Vesicourachal diverticulum
This is formed when the vesical end of the urachus remains unobliterated resulting in an outpouching from the urinary bladder dome anteriorly in the midline. The diverticulum usually has a broad neck and therefore is not generally associated with complications as there is no urinary stasis.
Imaging reveals (micturating cystourethrogram and Contrast enhanced CT) a tubular contrast-filled outpouching from the anterior bladder dome without any communication with the umbilicus.
Management
Symptomatic patients are usually treated surgically. Nowadays, however, symptomatic infants after birth may be treated conservatively with surgical treatment being employed only in cases with recurrent symptoms or when urachus fails to obliterate even at 1 year of age. Recommended operative treatment for urachal remnants is complete surgical excision of the remnant. Patent urachus and vesicourachal diverticulum extend up to the urinary bladder, and they thus require a bladder-cuff placement to avoid subsequent complications.
Associations
Urachal remnants may be associated with other genitourinary abnormalities like vesicoureteral reflux, hypospadias, meatal stenosis, crossed renal ectopia, umbilical or inguinal hernias, anal atresia, cryptorchidism, omphalocele and ureteropelvic obstruction.
Complications
Urachal remnants may give rise to the following complications:
1. Infection
2. Stone formation due to urinary stasis
Infection is the commonest complication occurring in patients with persistent urachal remnants. Most common organism found in these cases is Staphylococcus aureus. Infection can lead to abscess or fistula formation, which can rupture, resulting in peritonitis and sepsis. Ultrasonography reveals complex echogenicities within the usually clear anechoic urachal remnant. CECT in such cases shows a peripherally enhancing heterogeneous collection or lesion. Enterography with positive oral contrast and sonography may sometimes be indicated to rule out a urachoenteric fistula.
Neoplasms – These can be benign or malignant. Benign tumours are rare and can develop from any part of the urachal tract. Benign tumours that can arise from urachal remnants include adenomas, cystadenomas, fibromas, fibromyomas, fibroadenomas and hamartomas. Malignant neoplasms that can occur in urachal remnants include adenocarcinomas, urothelial carcinoma, squamous cell carcinoma. Adenocarcinomas are less than 1% of all bladder cancers. However, 80% of cancers occurring in urachal remnants are adenocarcinoma. Urothelial, squamous and sarcomatoid neoplasms account for the remaining 20% of cases. Urachal adenocarcinomas are commoner in middle age and older men as compared to women. When they do occur they usually present with haematuria or palpable suprapubic mass. They are generally large at presentation with extravesical extension and hence have a poor prognosis. USG in such cases show a heterogeneous midline lesion. CT and MR are used for confirmation of the diagnosis and to evaluate for exact extent of the lesion, associated lymphadenopathy and metastases if any. Seventy per cent of urachal adenocarcinomas are calcified with the calcifications generally present at the periphery of the lesion. Thus, the presence of calcification in a midline mass at the expected location of urachus should raise suspicion of a urachal adenocarcinoma. On MRI, these show heterogeneous signal on T1W and T2W sequences, showing a predominantly hyperintense signal on T2W images; and show postcontrast enhancement.
Imaging differentials
A persistent omphalomesenteric duct may mimic patent urachus. In the omphalomesenteric duct, there is a communication of the anomalous tract with the bowel and not the urinary bladder, which can be confirmed on a fistulography study.
Endometriosis in the bladder dome can mimic a urachal neoplasm. Urachal adenocarcinomas can also be mistaken as primary urinary bladder malignancy or carcinoma of the other pelvic organs.
The vesicourachal diverticulum on imaging needs to be differentiated with postsurgical collections and simple urachal diverticulum. Characteristic midline location and communication with the bladder on cystography study helps in confirming this entity.
Infection and inflammatory conditions of urinary bladder
Etiopathogenesis: Acute cystitis most commonly occurs in women. It is defined as the infection of the bladder’s mucosal lining. Sexual intercourse and the use of spermicidal agents are some of the risk factors. Recent instrumentation, urinary bladder catheterization, bladder outlet obstruction, vesical calculi and neurogenic bladder facilitate the colonization of bacteria in the urinary bladder wall. Escherichia coli is the commonest cause of acute cystitis. Patients experience burning micturition, dysuria, suprapubic tenderness and even haematuria. Microscopic analysis of urine will reveal more than 1,00,000 per ml of bacteria in urine and the presence of pus cells.
Imaging findings: History, clinical examination and laboratory investigations are adequate for the diagnosis of cystitis. Patients are usually referred for imaging to confirm the diagnosis and assess for predisposing conditions. Imaging may also serve as primary diagnostic modality if the patient presents with vague symptoms. Ultrasound requires an adequately distended urinary bladder to evaluate for cystitis. It shows urinary bladder wall thickening (>5 mm) and moving internal echoes. Care should be taken to look for renal, ureteric or bladder calculus and presence of any bladder diverticulum. Bladder outlet obstruction if present, may reveal thickened bladder wall with the presence of sacculations and trabeculations. Abdominal radiographs can be done to look for stones. Plain CT may also be performed for urinary calculi. The reporting radiologist should include the number, site of calculi and the CT attenuation values of the calculi in the report.
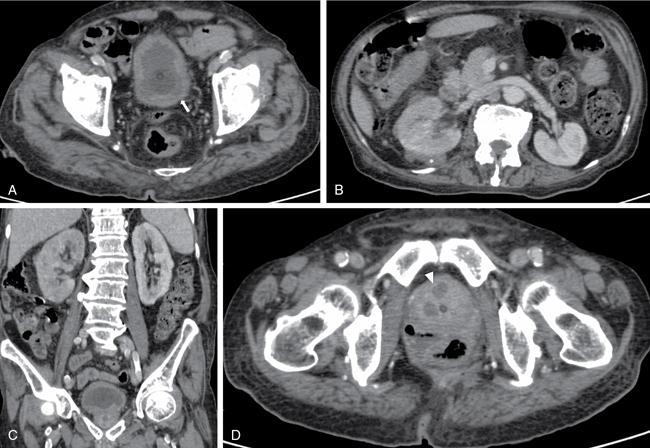
Fig. 10.13.3Acute cystitis, prostatic abscess and right sided pyelonephritis: Contrast enhanced CT Abdomen study of a 75-year-old male patient with burning micturition and fever spikes. Figure A demonstrates the irregular thickening of the urinary bladder (white arrow). Figure B and C show bulky right kidney with perinephric collection (white asterisk in B) suggestive of right pyelonephritis. Figure D shows peripherally enhancing collections within the prostate suggestive pf prostatic abscesses (white arrowhead).
Eosinophilic cystitis
Etiopathogenesis: Eosinophilic cystitis is an uncommon, chronic inflammatory disease involving the urinary bladder affecting both children and adults with a slight male predominance. Pathologically, it is seen as transmural inflammation of the bladder wall with the lamina propria most severely affected. Varying degree of fibrosis and necrosis is also appreciated. It can be idiopathic or can be seen in association with an adverse reaction to drugs or food, parasitic and nonparasitic bladder infection, autoimmune diseases, bladder carcinoma and eosinophilic enteritis. Patients may present with haematuria, dysuria or urinary retention. Cystoscopy may reveal erythema, polypoidal or ulcerative lesions and bladder masses.
Imaging findings: Urinary bladder wall in eosinophilic cystitis may be regular, normal or thickened. Single or multiple bladder masses can be seen which may be sessile. In the late fibrotic stage, the bladder is contracted and may be associated with hydronephrosis. On MRI, the bladder masses appear hyperintense relative to muscle on T1W and hypointense on T2W images. Enhancement is seen after intravenous gadolinium injection. A biopsy may be needed to rule out malignancy which may coexist with eosinophilic cystitis. Removal of causative agent results in a reversal of the disease process. However, transurethral resection of the bladder masses, coupled with antihistamine and steroid therapy, may be needed in a few cases.
Chemotherapy- and radiation-induced cystitis
Etiopathogenesis: Haemorrhagic cystitis may ensue after chemotherapy or radiotherapy. Chemotherapy-induced cystitis results from systemic or local therapy. Radiation-induced cystitis, on the other hand, results from external or intracavitary therapy for bladder or other pelvic malignancies. There is a breakdown of the urothelium resulting in haemorrhagic cystitis. The urothelium may then be covered with fibrinous exudates. When the bladder is severely affected, there may be bladder wall necrosis, incontinence, and fistula formation.
Imaging findings: On imaging, radiation or chemotherapy-induced cystitis manifests as diffuse irregular thickening of the bladder wall. In haemorrhagic cystitis, a blood clot may be seen within the bladder lumen and may be easily differentiated from a bladder mass on ultrasound because it is generally mobile. On CT, the clot appears hyperdense. If a bladder neoplasm cannot be ruled out, a limited scan covering the bladder may be performed in a prone position when the clot occupies the dependent part confirming its mobile nature. On MRI, the bladder wall is oedematous and appears hyperintense on T2W images. In chronic severe therapy-induced cystitis, the urinary bladder is contracted, because of fibrosis. Calcifications may be uncommonly seen. This may result in hydronephrosis. Chronic changes in pelvic irradiation include fatty infiltration of pelvic organs and enlargement of presacral space. Gas within the bladder lumen is suggestive of fistula formation, and a fluoroscopic or CT cystogram study may be required to demonstrate the fistulous tract. In CT cystography, diluted water-soluble iodinated contrast is instilled into the urinary bladder retrogradely. The contiguous axial sections at the level of the urinary bladder are then acquired, which may reveal contrast-filled curvilinear tract.
Only gold members can continue reading. Log In or Register to continue