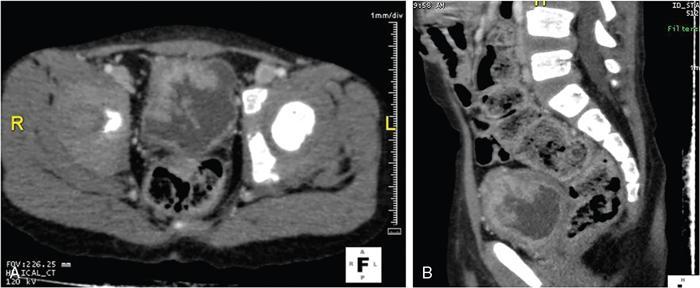
Anmol Bhatia, Kushaljit Singh Sodhi, Akshay Kumar Saxena Congenital as well as acquired anomalies of the bladder and urethra are a significant cause of morbidity in children. Various radiological investigations for imaging bladder and urethra include ultrasonography (US), voiding cystourethrography (VCUG) and intravenous urography (IVU), computed tomography (CT), magnetic resonance imaging (MRI) and contrast-enhanced voiding urosonography. In this chapter, we will discuss and illustrate a wide spectrum of congenital and acquired anomalies of bladder and urethral in children. Foetal allantoic stalk is the connection between the bladder dome and the umbilicus during the embryogenesis. Normally, it gets involuted by the second month of gestation. Depending on the degree of the persistence of this foetal allantoic stalk results in varying types of urachal remnants. The clinical presentation depends on the type of urachal remnant: Fluoroscopy is the best imaging modality for documenting the patency of urachus. However, there may be an underestimation of the exact length of the urachal remnant as inflammation occurring along the tract may block its lumen. CT and MRI are usually not needed for the detection of urachal remnants. However, urachal remnants are usually detected incidentally on CT scan done for other indications. Cystic or solid elongated tubular structure may be seen extending from bladder dome to umbilicus. A focal cystic lesion (Fig. 10.11.3) may be seen in the midline anywhere from bladder dome to umbilicus. In case the urachal remnant present with the symptoms, resection of the entire tract is warranted. Bladder diverticulum are localized outpouching from the bladder wall. They can be single or multiple of varying sizes. A male predominance is seen in comparison to females. It has been traditionally classified into four types: They can be incidentally detected or present with complications including recurrent UTI, urinary retention, incontinence, stone formation, VUR and bladder or ureteric obstruction. Bladder diverticulum should be differentiated from ‘bladder-ears’ in newborn male which is bilateral protrusion of bladder wall into inguinal ring. These are transient and disappear with growth. Appearance of diverticulum depends on cause, location, size and presence of complication features. VCUG under fluoroscopy is most efficient method to demonstrate diverticulum. Fluoroscopic monitoring during all phases including voiding and immediate postvoiding phase is important along with oblique and lateral views. Contained contrast-filled outpouching is seen which may be visible only during voiding phase when urine is forced into diverticulum during bladder contraction. Associated VUR is present in 50% of cases. Round or oval anechoic structure arising in communication with the bladder is seen. Well-defined homogenous structure with fluid attenuation/signal intensity arising from bladder wall (Fig. 10.11.6). Secondary complications like stone formation or rupture can be seen. Surgical removal using intravesical, extravesical or combined approach may be performed along with meticulous repair of bladder wall. Urinary bladder neoplasms are not commonly encountered in children. The majority of bladder neoplasms in children are of mesenchymal origin and overall rhabdomyosarcoma is the most common malignancy (Table 10.11.1). They can be incidentally detected or present with urological symptoms including dysuria, haematuria, incontinence and lower abdominal pain. It can manifest as filling defect in MCU studies done for other indications. Ultrasound is usually the first line investigation with cross-sectional imaging being performed in suspected cases for accurate characterization, localization, disease extent and complication. Histopathological analysis is often needed for final diagnosis. The differential diagnosis of bladder masses includes masses arising from adjacent pelvic structures, variants like ureterocoele or urachal remanent, mass forming cystitis (eosinophilic cystitis, BK virus–associated cystitis), haematoma, calculi or iatrogenic materials (e.g. Deflux used in VUR surgeries). Rhabdomyosarcoma Leiomyoma Neurofibroma IMT Leiomyosarcoma Angiosarcoma Haemangioma Urothelial carcinoma PUNLMP: urothelial papilloma Fibroepithelial polyp Paraganglioma Nephrogenic adenoma PUNLMP, papillary urothelial neoplasm of low malignant potential. Rhabdomyosarcomas are the most common urinary bladder neoplasms in first two decades of life presenting typically at ages 2–6 years and 15–19 years. Syndromic association with Li–Fraumeni cancer syndrome, NF type 1, MEN 2A has been found; however, majority are sporadic in origin. Histological subtypes include embryonal rhabdomyosarcoma (classical, botryoid and spindle cell variant), alveolar and undifferentiated sarcoma types of which embryonal form accounts for 90% of all cases. Locoregional spread to adjacent organs, muscles, regional lymphnodes is seen with distal metastasis to lung, cortical bones and retroperitoneal lymphnodes. Metastasis is found in approximately 10%–20% of patients at time of initial presentation. Overall survival and outcome depend on patient age and histological subtype with patients between 1–9 years of age and embryonal subtype having a better prognosis. Imaging work-up includes CT or MRI pelvis for local disease characterization and extent, CT chest, bone scintigraphy or FDG-PET for metastasis and staging. They commonly arise from bladder trigone and neck area. Ultrasound: They are typically large, intraluminal, multilobulated masses with well-defined margins and homogenous hypoechoic or hyperechoic echotexture. Foci of necrosis or haemorrhage are often seen. Vascularity on colour Doppler is increased. Hydronephrosis and bladder neck obstruction secondary to mass can be found. CT: Bulky heterogenous low attenuation mass that may invade into periurethral or perivesical tissue (Fig. 10.11.7). Calcification is rare.
10.11: Bladder and urethral abnormalities in children
Introduction
Urachal anomalies
Introduction
Types
Presentation
Imaging
Fluoroscopy
Cross-sectional imaging (CT/MRI)

Treatment
Bladder diverticula
Introduction

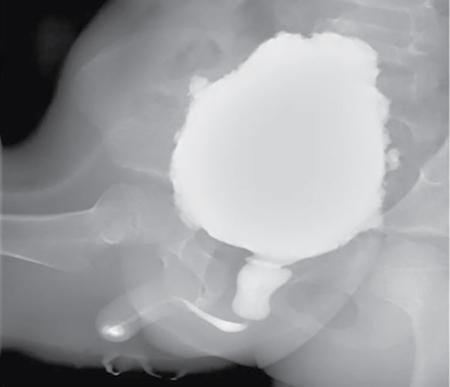
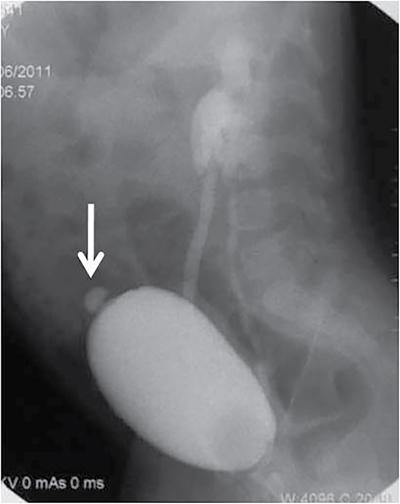
Imaging
Fluoroscopy
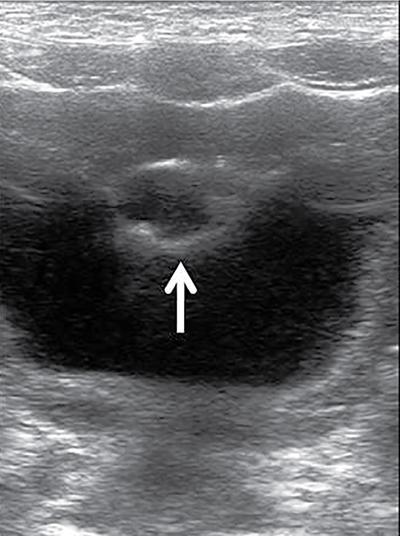
Ultrasound
CT and MRI

Treatment
Neoplasms
Histological Tumour Type
Tumours
Mesenchymal tumours
Urothelial tumours
Neurogenic tumour
Glandular bladder lesions
Mesenchymal neoplasms
Rhabdomyosarcoma
Introduction.
Imaging.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


