Boerhaave Syndrome
Michael P. Federle, MD, FACR
Key Facts
Imaging
Sudden increase in intraluminal pressure leads to full thickness esophageal perforation
Usually from left side of distal thoracic esophagus
Chest film
Left side pleural effusion or hydropneumothorax
Radiolucent streaks of gas along aorta or in neck
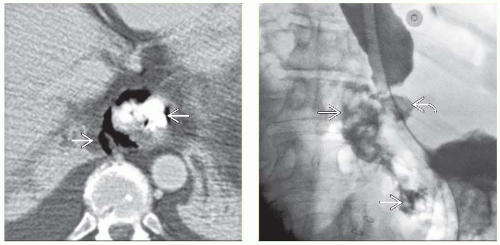
Esophagography with nonionic, water-soluble contrast agent
Shows extravasation of ingested or injected (through NG tube) contrast medium
From left side of esophagus, just above GEJ
CT
Extraluminal gas &/or oral contrast medium in lower mediastinum ± upper abdomen
Protocol advice
Plain chest radiograph; helical CECT with oral contrast
Esophagography with nonionic water-soluble contrast agent
If initial study with water-soluble contrast medium fails to show leak; examination must be repeated immediately with barium to detect subtle leaks
Clinical Issues
Accounts for 15% of total esophageal perforation cases
Prognosis for large perforation
After 24 hours without treatment: Mortality = 70%
After immediate surgical drainage: Good
Treatment
Drains in esophagus, mediastinum, pleural space, ± abdomen
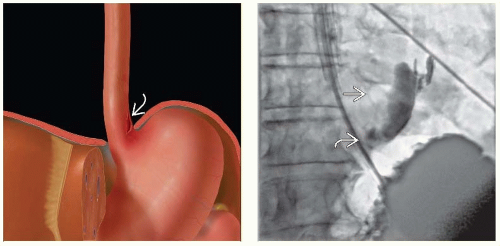 (Left) Graphic shows a vertically oriented laceration  of the distal esophagus, just above the hiatus and GE junction. (Right) Film from an esophagram, following injection of water-soluble contrast medium through a nasogastric tube, demonstrates a leak of contrast medium of the distal esophagus, just above the hiatus and GE junction. (Right) Film from an esophagram, following injection of water-soluble contrast medium through a nasogastric tube, demonstrates a leak of contrast medium  from a tear in the left anterior wall of the distal esophagus from a tear in the left anterior wall of the distal esophagus  , a classic appearance for Boerhaave syndrome. , a classic appearance for Boerhaave syndrome. |
 (Left)
Get Clinical Tree app for offline access
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|