8 Bone Imaging Diana Gaitini, Daniela Militianu, Alicia Nachtigal, and Vikram S. Dogra
 The Physics of Bone Imaging
The Physics of Bone ImagingAlthough the medullary bone cannot be demonstrated on ultrasound, the sharp definition of cortical bone contours enables normal and pathologic bone diagnoses to be performed based on this modality.
According to the physics of ultrasound, the amount of sound reflection (R) or backscatter is determined by the differences in acoustic impedances (Z) of the tissues or materials forming the interface [e.g., (ΔZ) between Z 2 and Z1]. Acoustic impedance of a tissue (Z) is directly proportional to density (p) and sound propagation velocity (c)
Z = p . c
For different media, the acoustic impedance changes considerably. For example, for air, Z = 0 (p ≅0 and c = 340 m/s); for muscle, Z = 1.65 (p = 1.06 g/cc and c = 1.560 m/s). The acoustic impedance of bone is much higher than the one for soft tissues
Z= 8 (p= 2 g/cc and c = 4.000 m/s)
Sound reflection (R) is a function of the differences in acoustic impedances of the media at the interface:
R= Z 2 – Z1 / Z2 + Z1
At an air–tissue interface, R= 1 (R= 0 – 1.5 / 0 + 1.5), which means that all the incident sound is reflected. At a bone-tissue interface, which means that 70% of the incident sound is reflected.
R= 0.7 (R = 8 − 1.5 / 8 + 1.5)
From these equations, we may infer that the highly reflective tissue–bone interface is seen as a hyperechogenic line with posterior acoustic shadow.
 Technical Guidelines and Normal Anatomy
Technical Guidelines and Normal Anatomy
Transducer and Equipment Capabilities
High-resolution broad bandwidth 5 to 12 MHz or 4 to 8 MHz, when the depth of the scanned target exceeds 2 to 3 cm, linear array transducers or 5 to 8 MHz and even 2 to 5 MHz, when depth exceeds 4 to 5 cm, sector array transducers are currently used for bone sonography. With the development of software and hardware new technologies like tissue harmonic and extended field-of-view imaging, sharp definition of bone contours and the surrounding tissues may be achieved.
Patient Positioning
The patient is examined seated or lying down, according to the anatomic region to be scanned, allowing a comfortable positioning for patient and examiner. The examiner is generally seated on a wheeled chair in front of the patient.
Normal Anatomy
Ultrasound examination is able to identify bone contours, cartilage on articular surfaces, tuberosities, grooves, fossae, and other bone structures.
 Pathologies
PathologiesFractures
On ultrasound, fractures appear as focal breaks of the cortical hyperechogenicity, frequently associated with periosteal thickening and subperiosteal hematoma.
Linear Fracture
Disruption of the normal bone cortex is demonstrated on ultrasound by a step-off deformity or angulation of the fractured bones. Adjacent subperiosteal hemorrhage confirms the diagnosis (Fig. 8.1).
Subchondral Compression Fracture
Compression fractures of the humeral head are often hardly visualized on x–ray. A triangular-shaped defect in the cortex of the humeral head is detected on ultrasound. A Hill–Sachs fracture is the result of an impact of the humeral head on the glenoid contour in anterior shoulder dislocation. It is seen at the posterolateral contour of the humeral head (Fig. 8.2). A McLaughlin fracture is the homonymous of the previous one at the anterior humeral head contour (Fig. 8.3), developing as a result of a posterior shoulder dislocation. Large lesions are associated with a predisposition for recurrent dislocation.
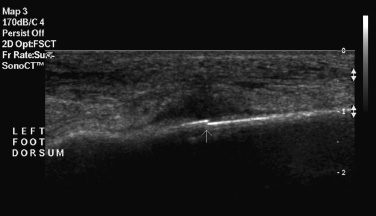
Fig. 8.1 Linear fracture. Step-off discontinuity of a metatarsal bone surface (small arrow) in a soldier with acute middle foot pain, compatible with stress fracture. Adjacent to the fracture, a sonolucent hematoma and soft tissue edema are seen.
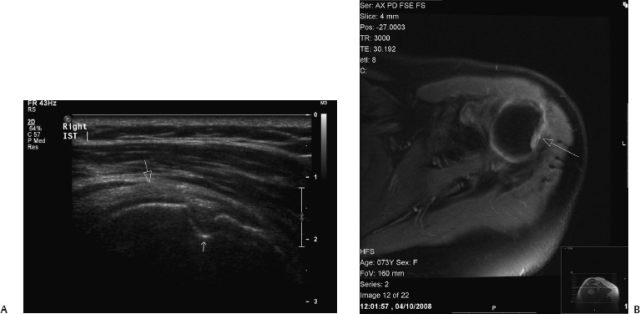
Fig. 8.2 Hill–Sachs compression fracture. (A) On ultrasound, a triangular notch representing an osteochondral fracture is seen at the posterior area of the humeral head (small arrow). The bone defect is filled by synovial fluid. The rotator cuff(large arrow) is seen above the humeral head. (B) Axial proton-density fast spin echo fat-suppressed magnetic resonance image (PD FSE FS MRI) shows the defect in the humeral head (arrow).

Fig. 8.3 McLaughlin compression fracture. Triangular defect in the anteromedial aspect of the humeral head (arrowheads). The bone defect is seen below the subscapularis (SSC) tendon.
An osteochondral fractured segment may be seen standing free in the proximity of a fractured bone (Fig. 8.4).
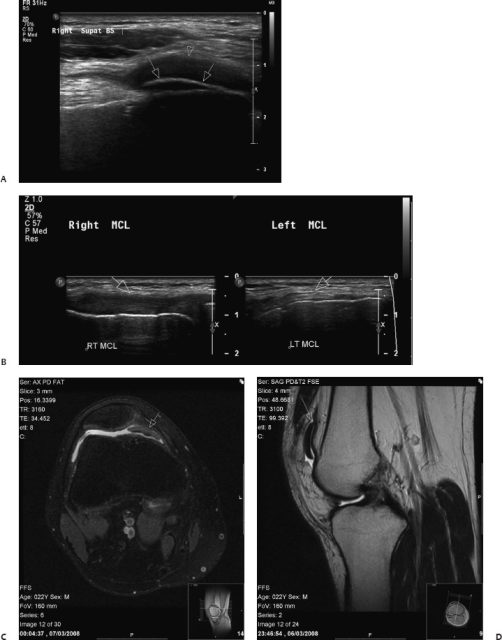
Fig. 8.4 Osteochondral avulsion fracture of the patella. (A) On ultrasound, a hyperechoic bone fragment is seen at the medial side of the right knee, due to avulsion fracture of the patella (arrows) with cranial displacement. Fluid is detected in the suprapatellar bursa (arrowhead). (B) Ipsilateral middle collateral ligament tear (arrow) secondary to trauma is seen on the left plot, opposite to the normal contralateral ligament (arrow) on the right plot. (C) Axial proton-density fast spin echo fat-suppressed magnetic resonance image (PD FSE FS MRI) shows the loose osteocartilage fragment (arrow) in the medial recess of the suprapatellar bursa, surrounded by synovial fluid. (D) On sagittal PD FSE MRI, the medially displaced osteocartilaginous fragment (arrow) may be seen.
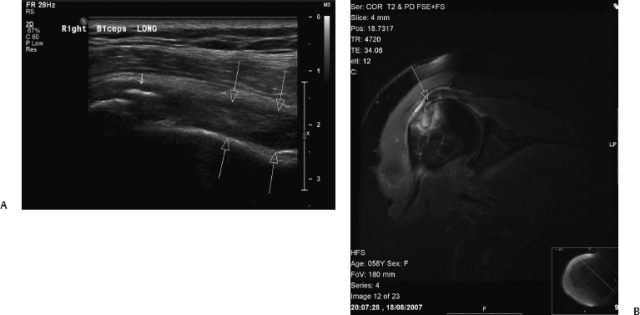
Fig. 8.5 Occult fracture at the humeral greater tuberosity. (A) Discontinuity in the normally smooth bony surface and avulsion fracture are seen on sagittal ultrasound. The osteochondral fragment is seen as a hyperechogenic focus (short arrow) at the proximal bicipital groove. A large hematoma is seen along the humeral shaft (long arrows), posterior to the long head of the biceps tendon. (B) On coronal MRI PD FSE FS a fracture line surrounded by intramedullary contusion and mild compression of the greater tuberosity (arrow) is seen.
Occult Fracture
Unsuspected fractures on conventional radiography may be diagnosed on ultrasound. Examples are a humeral greater tuberosity fracture (Fig. 8.5), which leads to impingement in the subacromial space, and fractures at ribs. An occult fracture should be looked for in cases presenting with subperiosteal hemorrhage (Fig. 8.6
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


