Coma
No motor response to painful stimuli (e.g., pressure on supraorbital nerve, painful stimulus to nail bed or sternum)
Absent brainstem reflexes
Pupils mid-size or dilated, no response to bright light
No oculocephalic reflex (no grimacing nor eye opening with deep pressure on both condyles of the temporomandibular joint)
No corneal reflex when wiping the cornea with cotton wool
No oculovestibular response toward the side of the cold stimulus when ice water is injected into the external ear canal
No cough reflex on bronchial suctioning
No gag reflex on stimulation of the posterior pharynx
Apnea
No respiratory effort when patient is disconnected from the ventilator and CO2 is allowed to at least 20 mmHg above baseline
Confirmatory Tests
The role of confirmatory tests differs among countries but they generally are indicated when a specific part of the clinical examination cannot be performed or is deemed unreliable (Table 18.2).
Table 18.2
Conditions that may interfere with the clinical diagnosis of brain death and may require ancillary tests
Severe facial or cervical spine trauma confounding cranial nerve assessment |
Preexisting pupillary abnormalities |
Toxic levels of CNS-depressant drugs or neuromuscular blockage agents |
Severe chronic pulmonary disease or obesity resulting in chronic retention of carbon dioxide |
In the United States, the choice of tests is left to the discretion of the physician. Confirmatory tests demonstrate either extinct brain function (electroencephalography, evoked potentials) or cessation of cerebral blood flow (cerebral angiography, radionuclide angiography, cerebral perfusion scintigraphy).
Cerebral Angiography
Four-vessel cerebral angiography has traditionally been the gold standard for documenting cessation of cerebral blood flow. The arterial circulatory arrest within the cranium develops in a distal-to-proximal direction as intracranial hypertension progresses. Thus, the level of contrast stop descends from the subarachnoid to the cervical levels (Fig. 18.1a–g). Cerebral angiography is conclusive if the flow in the posterior circulation ceases at the foramen magnum and at the petrosal portion of the carotid artery in the anterior circulation. The external carotid circulation generally is patent, and filling of the superior sagittal sinus may be delayed.
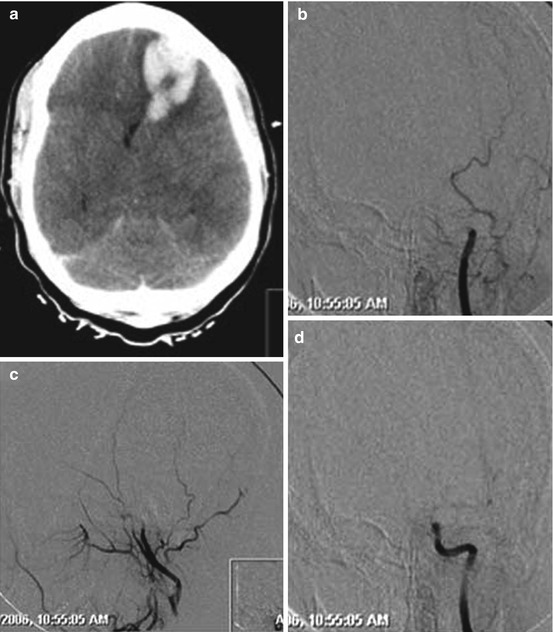
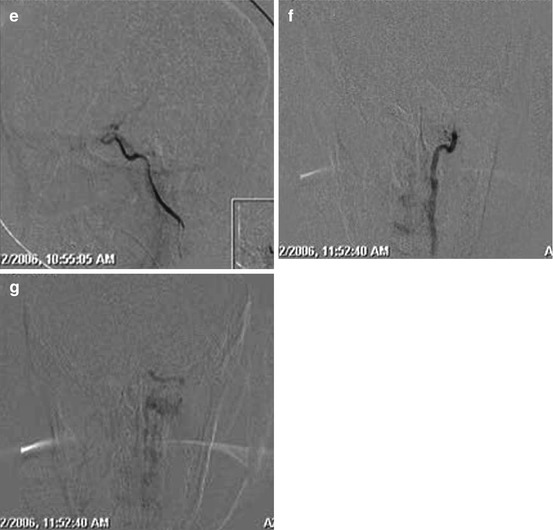
Fig. 18.1




Non-contrast computed tomography scan of the head (a) in an anonymous young female who was found comatose and tested positive for multiple drugs with evidence of a space-occupying left frontal lobar hemorrhage and diffuse brain edema. Cerebral angiography was pursued to rule out an underlying vascular anomaly. Left common carotid artery injection demonstrated cessation of flow distal to the supraclinoid segment of the left internal carotid artery in frontal (b, arterial phase; d, late capillary phase) and lateral plane (c, arterial phase; e, late capillary phase) leading to contrast stasis in the extradural segments of the left internal carotid artery. The left external carotid artery branches well opacified. Circulatory arrest at the foramen magnum was confirmed for the left vertebral artery (f, arterial phase; g, capillary phase) given the lack of opacification of any intradural segment of the left vertebral artery (Images courtesy of Darren B. Orbach, Interventional Neuroradiology, Boston Children’s Hospital)
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
