Fig. 1
Schematic drawing of two types of colorectal cancer. a Mass-forming colorectal cancer. b Short segmental wall thickening
Adjacent lymph node involvement is frequent and the liver is the most frequent site of distant metastasis.
3 Sonographic Findings of Colon Cancer
Sonographic features of colorectal cancer reflect its macroscopic pathology. Colorectal carcinoma classically appears as segmental thickening or as a bulky mass of the colonic wall with heterogeneous low echogenicity (Lim 1996).
Segmental wall thickening is usually short and asymmetric, eccentric or circumferential, with irregular contours (Fig. 2). This type of cancer is more frequently found in the left colon, where it determines narrowing of the lumen up to colonic obstruction. In this context, the lumen usually does not contain feces, but a small amount of gas, which may be also observed in the proximal pre-stenotic tract of the colon. Indeed, pre-stenotic tract may contain a large amount of fecal and gaseous content that may make the evaluation of the colonic walls more difficult (Fig. 3).
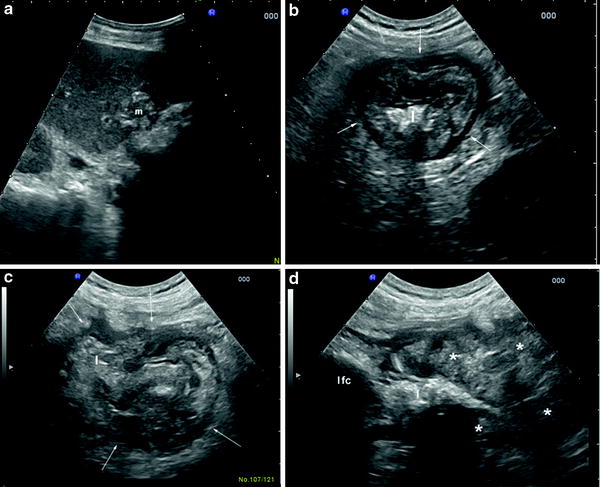
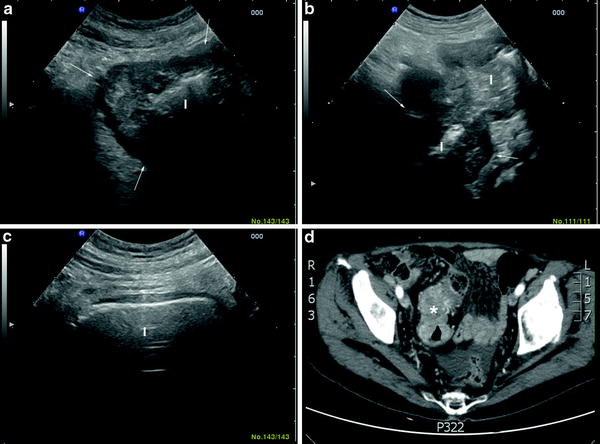
Fig. 2
Abdominal and intestinal ultrasound in a 76-year-old man presenting with alteration of liver function tests and abdominal discomfort. The abdominal ultrasound showed a solid lesion of the liver (m) suspected for metastasis from colorectal cancer (a). The following examination of the bowel, showed a lesion highly suspected for a carcinoma of sigmoid colon. In particular, transversal (b, c) and longitudinal (d) scans showed a segmental and asymmetric wall thickening (asterisks), with hypoechoic and dishomogeneous echo pattern. The bowel lesion showed was also characterized by irregular contours (arrows) with narrowing of the lumen (l) and prestenotic dilatation with solid fecal content (l fc)
Fig. 3
Sonographic aspect of a carcinoma of sigmoid colon. a Transversal scan shows a short segmental and asymmetric wall thickening with hypoechoic echo pattern (arrows); b longitudinal and c transversal scans showing the irregularity and the length of narrowed lumen (l) and the dilatation of the prestenotic segment (l), where fecal and gaseous content makes the evaluation of the colonic walls more difficult. d The same lesion detected by CT scan (asterisk)
The mass involving the colonic wall is more frequently found in the right colon. It may be variable in size, hypoechoic, and with irregular contours (Fig. 4). Often high echoes denoting intraluminal gas and feces may be visible within the mass, so that it appears as a “pseudokidney” (Fig. 5).
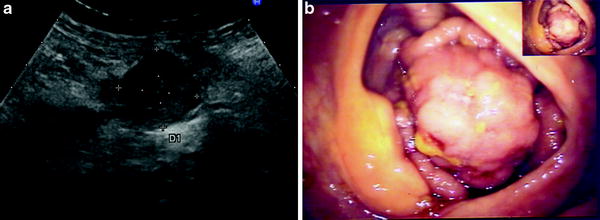

Fig. 4
Mass forming cancer of the cecum. a Ultrasound scan shows a well-defined, irregular mass (diameter 3 cm), representing an adenocarcinoma of the cecum. b The same lesion detected by colonoscopy
Fig. 5
Sonographic aspect of a carcinoma of ascending colon. Transversal scan shows a segmental and asymmetric wall thickening (asterisks) with hypoechoic echo pattern also called as “pseudokidney sign”. High echoes denoting intraluminal gas and feces may be visible within the mass (l)
The wall thickening with abrupt segmental loss of wall layer stratification and disappearance of haustra coli may be features of malignancy (Kuzmich et al. 2009) (Fig. 6; Video). Colonic wall may also show increased vascularity at color Doppler (Fig. 7). However, these signs are not specific, as they can also be observed in inflammatory diseases or colonic ischaemia (Lim 1996; Shirahama et al. 1994). Adjacent regional roundish hypoechoic lymphadenopathies should also be searched for because their presence may reinforce the suspicion of malignancy. Sonography of the liver should be performed as well to assess the presence of metastasis when a colorectal cancer is detected or suspected.
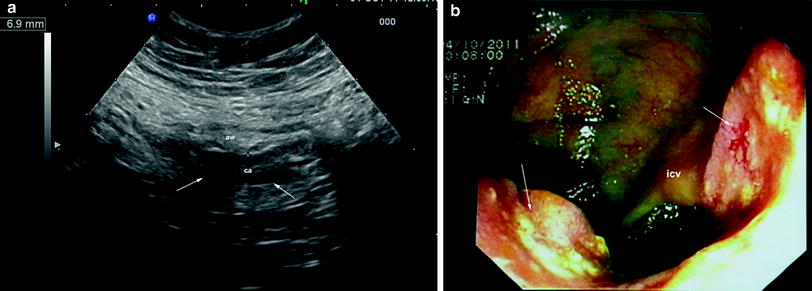
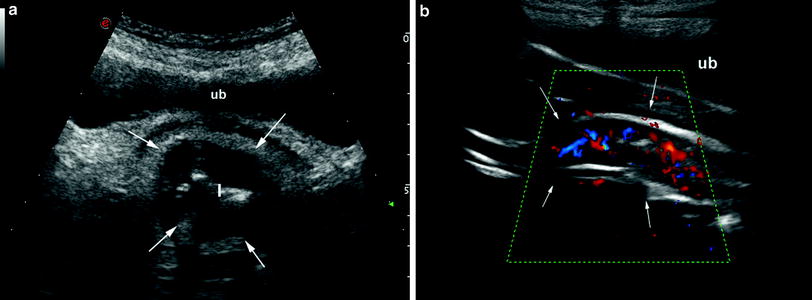
Fig. 6
56-year-old woman with abdominal discomfort and anemia. The bowel ultrasound showed a segmental thickening (ca) of the bowel walls (6.9 mm), with abrupt loss of stratification, in the ascending colon (arrows) (a). The following colonscopy showed an ulcerated colorectal cancer, involving half of the circumference of colon, just distal to the ileo-cecal valve (icv) (b). aw anterior wall of the ascending colon
Fig. 7
Carcinoma of the rectosigmoid junction. a Transverse ultrasonographic scan showing thickened hypoechoic walls (arrows). b Longitudinal ultrasonographic scan showing vascular signals within the bowel wall (arrows) at color Doppler denoting the hypervascularity of the lesion. Ub urinary bladder
However, it should be kept in mind that the absence of these findings at sonography does not exclude the diagnosis of colonic carcinoma. Small cancers and polyps can be overlooked, and the suboptimal diagnostic quality of the scan—due to bowel gas or obesity—can lead to false-negative results. On account of these limitations sonography is not an effective technique of screening for colonic cancer.
Several studies have evaluated the accuracy of transabdominal ultrasound in detecting colorectal cancer. Most of these studies showed that ultrasound detects accurately advanced colorectal tumors, included those causing colonic obstruction, but misses small cancers and polypoid lesions (Price and Metreweli 1988; Rutgeerts et al. 1991; Richardson et al. 1998; Grunshaw et al. 2000; Martínez-Ares et al. 2005; Gluvic et al. 2008). This has also been shown using transabdominal hydrocolonic sonography, namely the assessment of the colonic walls after bowel preparation with laxatives and following instillation of water into the colon (see “Oral Contrast-Enhanced Bowel Ultrasound




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
