Carcinoid
Todd M. Blodgett, MD
Alex Ryan, MD
Omar Almusa, MD
Key Facts
Terminology
Neuroendocrine tumor derived from enterochromaffin cells
Carcinoid, carcinoid syndrome (CS), carcinoid tumor
Imaging Findings
Primary bowel lesion with spiculated soft tissue mass in abdomen ± desmoplastic reaction ± calcifications
Hepatic or lung tumors in patient with CS
Chest mass: Endobronchial lesion with or without post-obstructive pneumonia
FDG PET: Sensitivity 75%
Generally low FDG uptake among neuroendocrine tumors
Atypical carcinoid can appear as a small pulmonary nodule with extensive hilar or mediastinal lymph node enlargement
Carcinoids tend to be vascular and can exhibit considerable enhancement
Helpful for differentiating tumor from obstructive atelectasis and adjacent mucous plugs
Whole-body morphologic imaging and somatostatin receptor scintigraphy best combination
Top Differential Diagnoses
Lymphoma
Other Neuroendocrine Tumors
Mesenteritis
Liver Metastases
Diagnostic Checklist
FDG PET or PET/CT may show only mild to moderate FDG activity within lesions
 Axial CECT shows a slightly spiculated mass in the small bowel mesentery with areas of calcifications  , most compatible with carcinoid. , most compatible with carcinoid. |
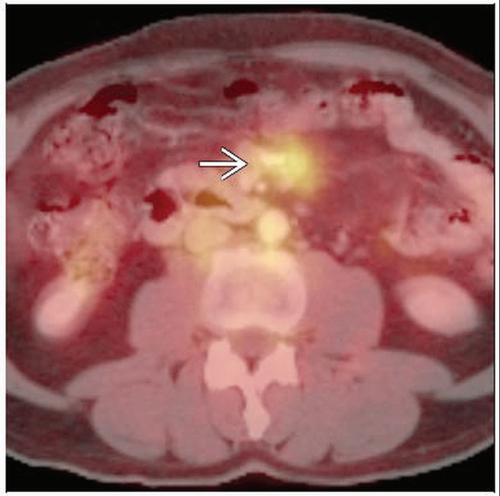 Axial fused PET/CT shows moderate FDG activity in the mesenteric mass  , compatible with carcinoid. , compatible with carcinoid. |
TERMINOLOGY
Abbreviations and Synonyms
Carcinoid, carcinoid syndrome (CS), carcinoid tumor
May indicate malignant or benign disease
Definitions
Neuroendocrine tumors arising from enterochromaffin cells of Kulchitsky
IMAGING FINDINGS
General Features
Best diagnostic clue
Variably calcified soft tissue mass in abdomen with spiculation and desmoplastic reaction
Often asymptomatic
Tumors of liver or lung in patients with carcinoid syndrome
Mass within bronchus with varying degrees of post-obstructive pneumonia
Location
Abdominal carcinoid common, specifically in large intestine and appendix
Primary carcinoids of bowel are often not seen with CT
Metastases are frequent from midgut tumor but rare from appendiceal primary
Thoracic carcinoid most commonly found within bronchial lumen
Also seen in lung parenchyma and peribronchiolar lymph nodes
Peripheral lung tumor may represent atypical pulmonary carcinoid, half of which show lymph node involvement or distant metastases
Size
May become bulky, up to 25 cm
Size generally correlates with malignant behavior
Tumors < 1 cm metastasize in 2% of cases
Tumors 1-2 cm in 50% of cases
Tumors > 2 cm in 85% of cases
Volume may not change following treatment despite good clinical response
Morphology
Thoracic carcinoid highly vascular with no characteristic calcification distribution
Atypical carcinoid: Small peripheral nodule surrounded by extensive hilar/mediastinal lymphadenopathy
Abdominal carcinoid typically manifests as homogeneous mesenteric mass with spiculation and variable calcification
Primary bowel lesion often not identified
Thickened neurovascular bundles may present as stellate or curvilinear fibrosis radiating from lesion and distorting surrounding bowel
Imaging Recommendations
Best imaging tool
Whole-body morphologic imaging and somatostatin receptor scintigraphy
SUV on FDG PET generally correlates with aggressiveness of tumor
Protocol advice
Somatostatin receptor imaging (SRI)
Administer 6 mCi (222 MBq) In-111 pentetreotide IV
Image with 173 keV and 247 keV photopeaks of In-111
Administer mild bowel cathartic to decrease colon accumulation in patients not experiencing diarrhea
Urinary bladder should be emptied prior to imaging to avoid obscuring pelvic findings
CT Findings
General
CT has shown superiority to octreotide scan for characterization of primary tumor and liver metastases
Benign and malignant disease cannot reliably be differentiated with CT
Half of indeterminate lesions are benign on biopsy
Carcinoid tumor highly vascular
Distinguishable from obstructive atelectasis and mucous plugs on contrast-enhanced images
Chest
Small pulmonary nodule with extensive hilar/mediastinal lymphadenopathy is classic finding for atypical carcinoid
Central carcinoids more commonly have variable calcification (˜ 1/3 of cases)
No pathognomonic pattern of calcium distribution known
Less commonly seen in peripheral tumors
CECT
Typical carcinoid
Homogeneous, smooth-bordered lesion
Highly vascular tumor with intense contrast enhancement
Atypical carcinoid
Generally larger tumors
May show central necrosis and be associated with hilar lymphadenopathy
Abdomen
Submucosal lesions
Vascular lesions enhance intensely
Mural nodules more clearly visualized with water contrast
Well-defined morphology
Small bowel carcinoid
Masses are soft-tissue attenuation of variable size
Radiating stranding and border spiculation common
Retractile mesenteritis and treated lymphoma may share appearance, with calcification and desmoplastic reaction
Bowel loop ischemia may present as wall thickening and submucosal edema
Extension to mesentery
Homogeneous or heterogeneous ill-defined mass with spiculations and variable calcification
Desmoplastic reaction presents with finger-like extension into adjacent mesentery
Variable encasement and narrowing of mesenteric vessels
Fibrosis and desmoplastic reaction leads to fixation and obstruction of small bowel
Some tumors demonstrate cystic density
Metastasis to liver
Hypoattenuating on NECT
Strongly enhancing on CECT
Delayed images may show lesion isodense to liver
Often multiple
Colonic extension
Extraluminal mass common and better delineated on CT
Colon carcinoid has similar CT findings to adenocarcinoma, including a discrete mass or focal wall thickening
Nuclear Medicine Findings
Metabolic activity related to carcinoid in abdomen may be evaluated with several radionuclides: In-111 pentetreotide (Octreoscan), I-123/I-131 MIBG, FDG PET
FDG uptake generally low among carcinoid (and other neuroendocrine tumors)
May help differentiate pulmonary carcinoid from primary lung cancer
High suspicion for carcinoid in patients with clinical suspicion and low-uptake pulmonary nodule
SUV shown to correlate with aggressiveness of tumor; uptake correlates with mitotic figure and tumor proliferation
Overall PET/CT sensitivity 75%; specificity very low unless classic carcinoid syndrome is presentRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


