Cardiac Masses
QUESTIONS
A. The left atrium
B. The left ventricle
C. The right atrium
D. The right ventricular outflow tract (RVOT)
E. The aorta
View Answer
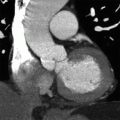
1a Answer B. Coronal postcontrast image shows a mass along the inferior apical left ventricular cavity. Left atrium is not shown in this image. Right atrium appears grossly normal. RVOT is not fully seen but appears normal. Visualized ascending aorta appears normal.
1b What is the best treatment for this lesion?
A. Surgical resection
B. Chemotherapy
C. No treatment
D. Anticoagulation
View Answer
1b Answer D. Left ventricular thrombus is most often associated with postinfarct wall motion abnormalities. Note the enhancement along the infarcted myocardium while there is no enhancement of the mass. Treatment of choice is anticoagulation. This is not a mass that requires surgical resection or chemotherapy. Treatment is necessary to prevent complications of thrombus embolization.
1c What is the most common type of mass seen in the heart?
A. Myxoma
B. Angiosarcoma
C. Thrombus
D. Rhabdomyoma
E. Melanoma
View Answer
1c Answer C. The most common mass in the heart is thrombus. The most common benign cardiac tumor is myxoma. The most common malignant tumor is angiosarcoma. The most common tumor in children is rhabdomyoma. Melanoma can metastasize to the heart but is not the most common cause of cardiac mass.
References: Grebenc ML, Rosado de Christenson ML, Burke AP, et al. Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation. Radiographics 2000;20(4):1073-1103; quiz 1110-1111, 1112. Review. PubMed PMID: 10903697.
Sparrow PJ, Kurian JB, Jones TR, et al. MR imaging of cardiac tumors. Radiographics 2005;25(5):1255-1276. Review. PubMed PMID: 16160110.
A. Aorta
B. Pulmonary artery
C. Pulmonary vein
D. Left atrium
E. Left atrial appendage
View Answer
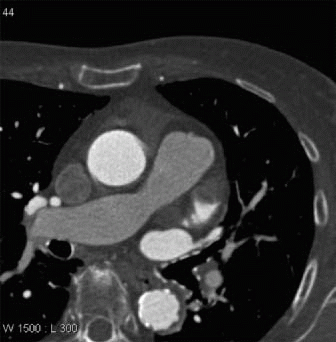
2a Answer E. Postcontrast gated coronary CTA shows a low-attenuation filling defect at the tip of the left atrial appendage. The aorta and pulmonary artery appear normal. Left atrium is only partially visualized along with the pulmonary veins, and they appear normal.
A. It is still there.
B. There is no abnormality.
C. The abnormality embolized.
View Answer
2b Answer B. The filling defect seen on the initial CTA at the tip of left atrial appendage is no longer identified on the delayed acquisition image. This is consistent with slow flow in the left atrial appendage, which can be seen in patients with atrial fibrillation and LA enlargement. Thrombus would have shown a persistent low-attenuation filling defect at the tip of the left atrial appendage with a border. It is unlikely that the thrombus could have embolized in the short amount of time between the initial CTA and the second acquisition.
2c What modality is most often used to evaluate for left atrial appendage thrombus?
A. CTA
B. MRI
C. Transesophageal echocardiogram
D. Transthoracic echocardiogram
View Answer
2c Answer C. Left atrial appendage thrombus is most often evaluated by transesophageal echocardiogram (TEE). While CTA can visualize LA appendage thrombus, its specificity is not high given false positives can happen with slow flow. A delayed phase may be helpful but adds additional radiation. MRI can also visualize left atrial appendage thrombus but is not used routinely as TEE is more available and performed just prior to pulmonary vein ablation.
Reference: Saremi F, Channual S, Gurudevan SV, et al. Prevalence of left atrial appendage pseudothrombus filling defects in patients “with atrial fibrillation undergoing coronary computed tomography angiography. J Cardiovasc Comput Tomogr 2008;2(3):164-171. doi: 10.1016/j.jcct.2008.02.012. Epub 2008 Mar 4. PubMed PMID: 19083941.
3 Left ventricular thrombus is most often seen in the setting of
A. Hypercoagulable state
B. Postinfarct
C. Infective endocarditis
D. Postsurgery
View Answer
3 Answer B. Left ventricular thrombus is most often associated with postinfarct wall motion abnormalities. Treatment of thrombus is anticoagulation. Surgical resection is not indicated and thrombus does not enhance following contrast administration. Left ventricular thrombus can be seen in hypercoagulable state, endocarditis, and postsurgery but is most often due to wall motion abnormality.
Reference: Keren A, Goldberg S, Gottlieb S, et al. Natural history of left ventricular thrombi: their appearance and resolution in the posthospitalization period of acute myocardial infarction. J Am Coll Cardiol 1990;15(4):790-800. PubMed PMID: 2307788.
4 Left atrial appendage thrombus is most often associated with
A. Lung cancer
B. Hypercoagulable states
C. Infarct
D. Atrial fibrillation
View Answer
4 Answer D. Left atrial appendage thrombus is most often associated with atrial fibrillation. While LA thrombus can occur with lung cancer invasion, it usually will occur via pulmonary vein extension and not occur at the tip of left atrial appendage. Thrombus can also occur in setting of wall motion abnormality (postinfarct, mitral valve replacement). While hypercoagulable states can predispose one to thromboembolic disease, it is not the most often cause of LAA thrombus.
Reference: Romero J, Husain SA, Kelesidis I, et al. Detection of left atrial appendage thrombus by cardiac computed tomography in patients “with atrial fibrillation: a meta-analysis. Circ Cardiovasc Imaging 2013;6(2):185-194. doi: 10.1161/CIRCIMAGING.112.000153. Epub 2013 Feb 13. Review. PubMed PMID: 23406625.
A. Thrombus
B. Metastasis
C. Myxoma
D. Infection
E. Lymphoma
View Answer
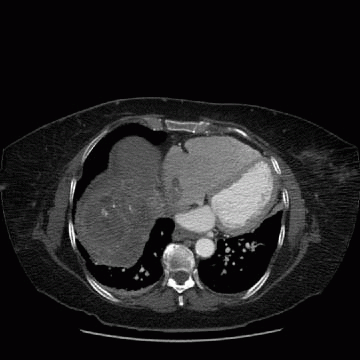
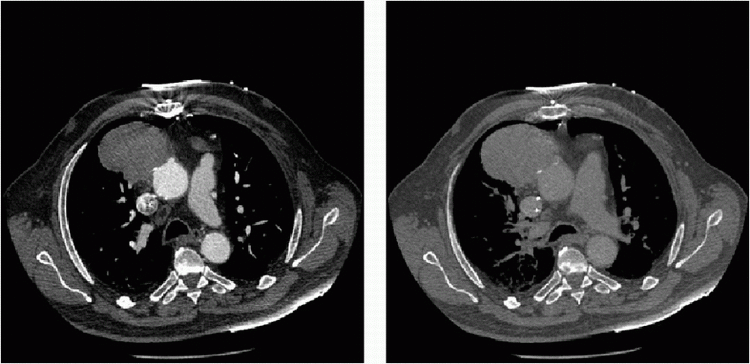
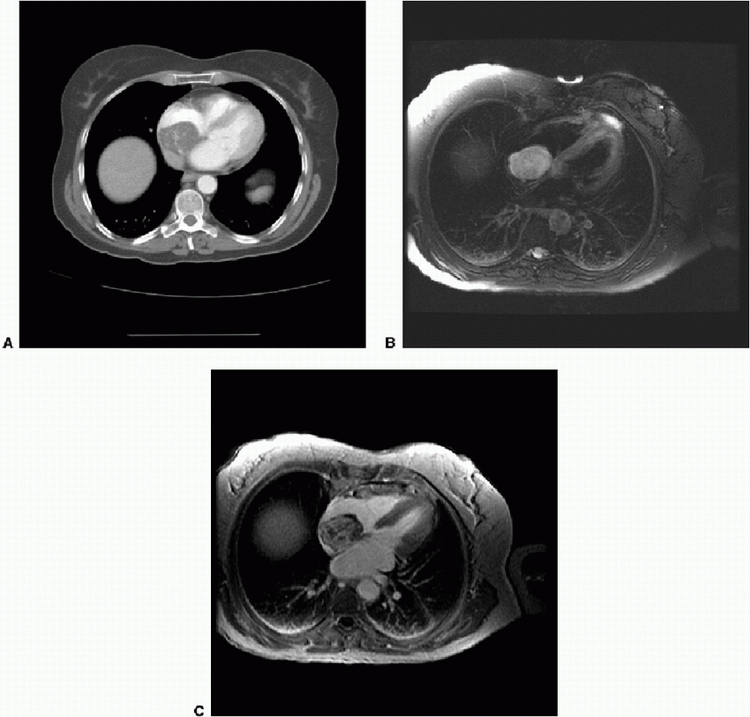
5 Answer B. While the most common type of mass in the heart is thrombus, in this case, there is evidence for metastatic disease (see liver lesions). This patient had hepatocellular carcinoma (HCC) with tumor invasion via the hepatic veins to the right atrium. Other tumors besides HCC with direct invasion to the right atrium include renal cell carcinoma and IVC sarcoma. Myxoma is within the differential and can be in the right atrium, but the liver lesions here make it more likely that this is a metastatic tumor. Endocarditis can cause masses in the valves, but they tend not to be this large. Lymphoma could also cause a mass in the heart but is not the best answer in this case given the liver findings.
References: Grebenc ML, Rosado de Christenson ML, Burke AP, et al. Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation. Radiographics 2000;20(4):1073-1103; quiz 1110-1111, 1112. Review. PubMed PMID: 10903697.
Sparrow PJ, Kurian JB, Jones TR, et al. MR imaging of cardiac tumors. Radiographics 2005;25(5):1255-1276. Review. PubMed PMID: 16160110.
A. Catheter angiography
B. Biopsy
C. Surgical resection
D. CABG
E. Medical treatment/chemotherapy
View Answer
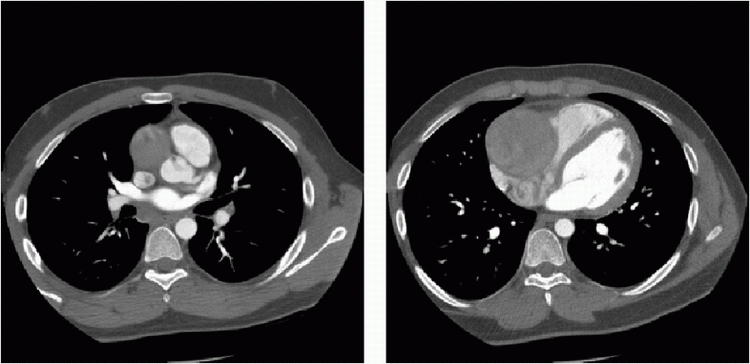
6 Answer E. This is a patient with metastatic lung cancer with likely vascular invasion (the mass appears to involve the aorta). The patient is already post-CABG (see sternotomy wires and bypass grafts). Saphenous graft aneurysm is also in the differential. However, note the heterogeneous enhancement of mass and irregular border, which would be more supportive of a mass such as lung cancer. Given that this is metastatic disease with likely vascular invasion, surgical intervention would not be indicated. While biopsy is a valid choice, if the differential includes saphenous aneurysm, then biopsy would not be a wise choice.
Reference: Gay SB, Black WC, Armstrong P, et al. Chest CT of unresectable lung cancer. Radiographics 1988;8(4):735-748. PubMed PMID: 3175085.
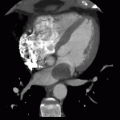
7 An 18-year-old male presents with chest pain and history of febrile illness. What is the next step?
|
A. Catheter angiography
B. CT-guided biopsy
C. Chemotherapy
D. Cardiac MRI
View Answer
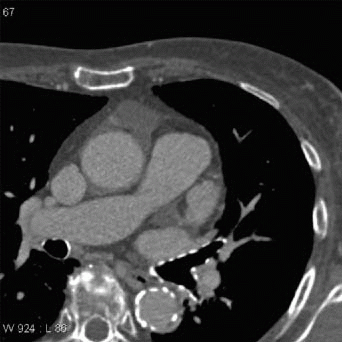
7 Answer A. This mass is most consistent with a large RCA aneurysm given the history suggesting Kawasaki disease. Catheter angiography is the best next step to better evaluate this aneurysm. One could argue for CABG right away if the diagnosis of giant RCA aneurysm was not in doubt. However, sometimes, the anatomy can be significantly distorted on CT that a catheter angiogram can show the aneurysm better than CT given the ability to directly inject the vessel. Biopsy would not be a wise choice for an aneurysm. Given this is not a tumor, medical treatment would not be helpful. CMR would not provide any more information given the findings are highly suggestive of giant RCA aneurysm already.
Reference: Díaz-Zamudio M, Bacilio-Pérez U, Herrera-Zarza MC, et al. Coronary artery aneurysms and ectasia: role of coronary CT angiography. Radiographics 2009;29(7):1939-1954. doi: 10.1148/rg.297095048. Review. PubMed PMID: 19926755.
A. No abnormality
B. Right lower lobe
C. Ascending aorta
D. Right heart border
E. Left atrium
View Answer
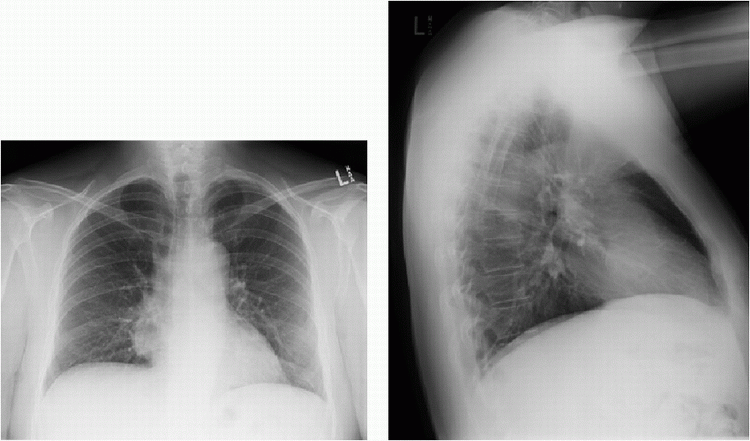
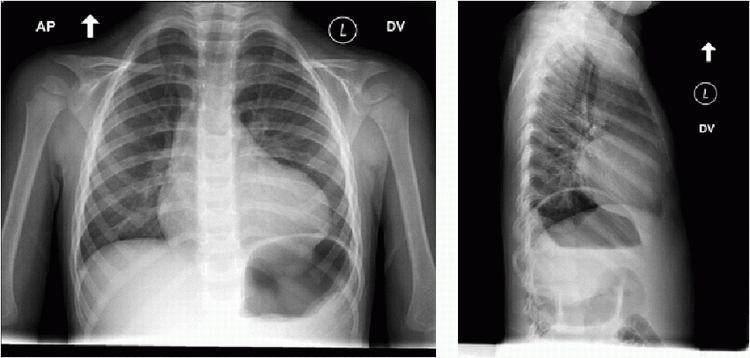
8a Answer D. The contour abnormality is at the right heart border on the PA view. The lateral view shows it adjacent to the heart and not posterior in the right lower lobe.
A. No treatment
B. Surgical resection
C. Serial MRI
D. Chemotherapy
View Answer
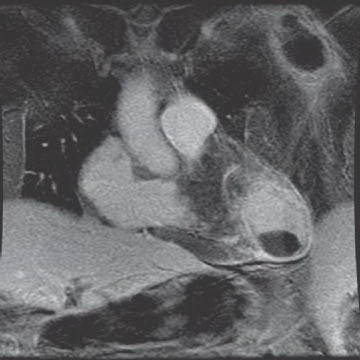
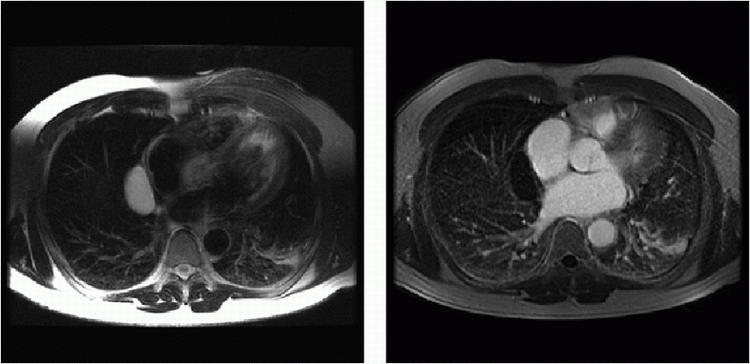
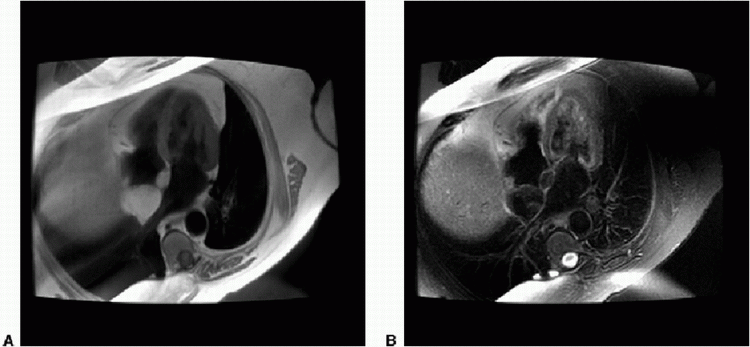
8b Answer A. This is right pericardial cyst along the right atrial border. It shows T2 prolongation on the T2W image. This mass shows no enhancement, septations, or nodules. Simple pericardial cysts do not require treatment or follow-up.
Reference: Restrepo CS, Vargas D, Ocazionez D, et al. Primary pericardial tumors. Radiographics 2013;33(6):1613-1630. doi: 10.1148/rg.336135512. Review. PubMed PMID: 24108554.
A. Anticoagulation
B. Chemotherapy
C. Surgery
D. Endovascular thrombolysis
View Answer
9 Answer C. This is a right atrial mass showing T2 prolongation (Image B) and heterogeneous contrast enhancement (Image C). While thrombus is the most common mass in the right atrium, in this case, the contrast enhancement excludes thrombus. The T2 prolongation and enhancement is suggestive of a right atrial myxoma. The best treatment is therefore surgery.
Reference: Grebenc ML, Rosado-de-Christenson ML, Green CE, et al. Cardiac myxoma: imaging features in 83 patients. Radiographics 2002;22(3):673-689. Review. PubMed PMID: 12006696.
A. Right atrial location
B. Sparing of fossa ovalis
C. Fluid suppression
D. Lack of enhancement
View Answer
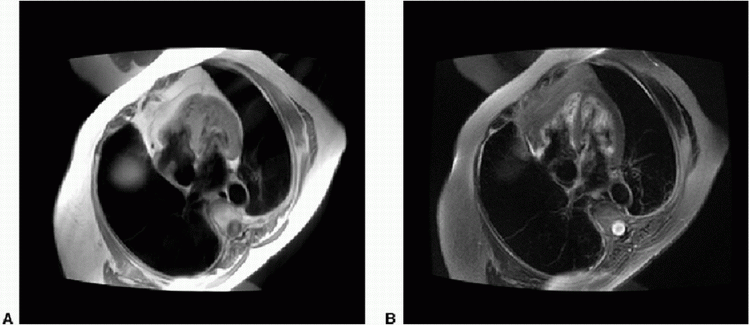
10 Answer B. Proton density-weighted (Image A) and post fat-saturated T2W (Image B) images show lipomatous hypertrophy of the interatrial septum (LHIAS). There is a classic barbell shape of the fat in the interatrial septum sparing the fossa ovalis. The right atrial location does not indicate a benign lesion as malignant and metastatic tumors can occur in this chamber. Fat suppression is used here, not fluid suppression. The images are noncontrast images so nothing can be said about the lack or presence of enhancement.
Reference: Kimura F, Matsuo Y, Nakajima T, et al. Myocardial fat at cardiac imaging: how can we differentiate pathologic from physiologic fatty infiltration? Radiographics 2010;30(6):1587-1602. doi: 10.1148/rg.306105519. PubMed PMID: 21071377.
A. Surgery
B. Anticoagulation
C. Chemotherapy
D. No treatment is necessary.
View Answer
11a Answer D. Proton density-weighted (Image A) and fat-saturated T2W (Image B) images show a right atrial wall mass that loses signal on fat suppression. There is suggestion of a thin capsule. This is most consistent with a right atrial lipoma. No treatment is necessary. This is not a tumor or thrombus that requires anticoagulation or chemotherapy or surgery. Lipomatous hypertrophy of the interatrial septum (LHIAS) can be positive on PET, but the lesion in this case does not involve the interatrial septum and appears to be a simple right atrial lipoma.
Reference: Kimura F, Matsuo Y, Nakajima T, et al. Myocardial fat at cardiac imaging: how can we differentiate pathologic from physiologic fatty infiltration? Radiographics 2010;30(6):1587-1602. doi: 10.1148/rg.306105519. PubMed PMID: 21071377.
11b What is an advantage of inversion recovery fat suppression over chemical fat suppression?
A. It is specific for fat.
B. It does not suppress contrast enhancement.
C. It does not require high field strength.
D. It is inherently high in signal.
View Answer
11b Answer C. Short tau inversion recovery (STIR) is not specific to fat as it will suppress anything with short T1 (including postcontrast T1 shortening). STIR imaging does not require a high field strength magnet. It will have lower signal due to the inversion pulse.
Chemical fat suppression is specific to fat and will not suppress contrast enhancement. However, it is susceptible to field inhomogeneity, which can cause incomplete fat saturation. With a higher-strength magnet, there is greater separation of the fat and water peaks making fat suppression easier.
Reference: Delfaut EM, Beltran J, Johnson G, et al. Fat suppression in MR imaging: techniques and pitfalls. Radiographics 1999;19(2):373-382. Review. Erratum in: Radiographics 1999;19(4):1092. PubMed PMID: 10194785.
12 Atrial and extracardiac myxomas can be seen in which condition?
A. Tuberous sclerosis
B. Von Hippel-Lindau
C. Multiple endocrine neoplasia (MEN)
D. Carney complex
E. Gorlin syndrome
View Answer
12 Answer D. Carney complex consists of multiple myxomas (including cardiac and extracardiac), endocrine neoplasm (pituitary adenoma), and skin hyperpigmentation. It is an autosomal dominant and is more common in females. The other syndromes do not include cardiac myxomas. In gorlin syndrome, patients have an increased risk for cardiac fibroma.
References: Ghadimi Mahani M, Lu JC, Rigsby CK, et al. MRI of pediatric cardiac masses. AJR Am J Roentgenol 2014;202(5):971-981. doi: 10.2214/AJR.13.10680. Review. PubMed PMID: 24758649.
Tao TY, Yahyavi-Firouz-Abadi N, Singh GK, et al. Pediatric cardiac tumors: clinical and imaging features. Radiographics 2014;34(4):1031-1046. doi: 10.1148/rg.344135163. PubMed PMID: 25019440.
A. Left atrium
B. Left ventricle
C. Right atrium
D. Right ventricle
View Answer




13a Answer B. The contour abnormality is along the left heart border, which is consistent with a LV abnormality.
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
