Carotid Dissection
Kenny E. Rentas
CLINICAL HISTORY
60-year-old male with acute onset of left-sided weakness and facial droop. The patient had recently been complaining of new right-sided headaches.
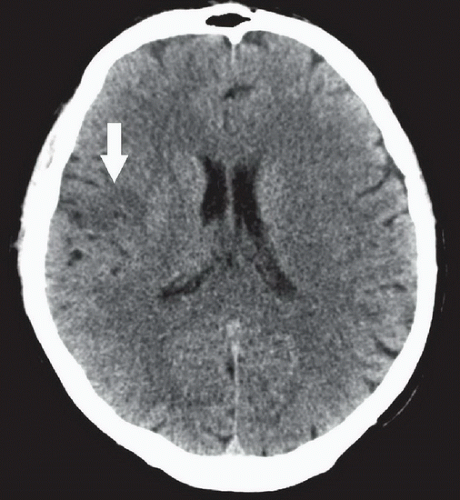 FIGURE 53A |
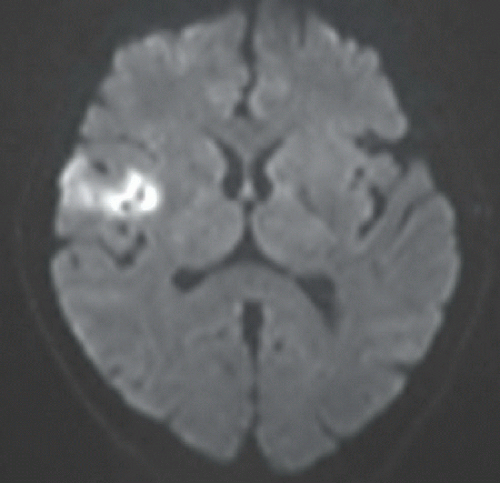 FIGURE 53B |
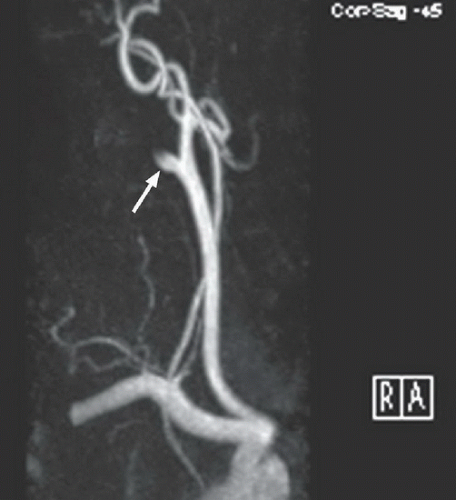 FIGURE 53C |
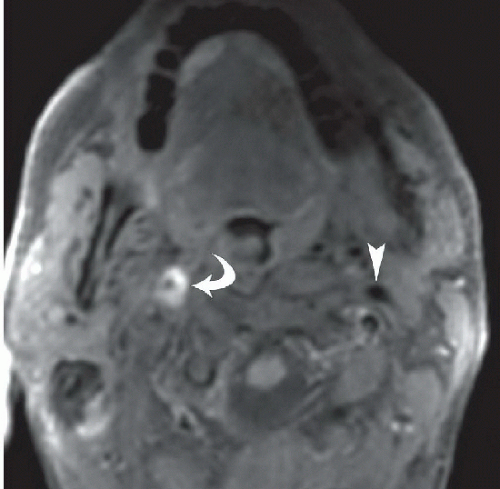 FIGURE 53D |
FINDINGS
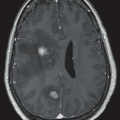
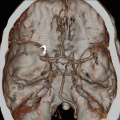
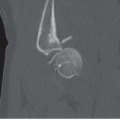
Figure 53A: Axial unenhanced CT image demonstrates an area of hypodensity in the right frontal lobe (large arrow) involving the cortex and subcortical white matter, concerning for cerebral infarction. Figure 53B: Axial DWI image demonstrates high signal intensity in this region, confirming the diagnosis of infarction. Figure 53C: Right anterior oblique 3D MIP image from a contrast-enhanced MRA of the neck demonstrates occlusion of the right internal
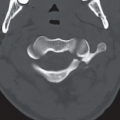
carotid artery (ICA; small arrow). The carotid bulb is relatively normal, and the vessel tapers proximal to the occlusion. Figure 53D: Axial fat-suppressed T1WI of the neck above the level of the carotid bifurcation demonstrates an eccentric crescent of high signal intensity encircling the lumen of the right ICA (curved arrow). Compare with the normal left ICA flow void (arrowhead).
carotid artery (ICA; small arrow). The carotid bulb is relatively normal, and the vessel tapers proximal to the occlusion. Figure 53D: Axial fat-suppressed T1WI of the neck above the level of the carotid bifurcation demonstrates an eccentric crescent of high signal intensity encircling the lumen of the right ICA (curved arrow). Compare with the normal left ICA flow void (arrowhead).
DIFFERENTIAL DIAGNOSIS
The primary differential in this case would be occlusion of the extracranial ICA secondary to atherosclerotic thrombosis or an arterial dissection. Atherosclerosis usually occurs in the elderly, affects multiple vessels, and commonly involves the vessel origin, carotid bifurcation, and carotid bulb. Arterial dissections usually spare the vessel origin, carotid bifurcation, and carotid bulb. Furthermore, dissections are usually solitary except in the setting of underlying vasculopathy or extensive trauma.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


