Cavernous sinus meningioma – immediate postoperative radiosurgery for perioptic residual
SKULL BASE REGION
Left cavernous sinus and middle cranial/infratemporal fossae
HISTOPATHOLOGY
Meningioma, WHO grade 1
PRIOR SURGICAL RESECTION
Yes
PERTINENT LABORATORY FINDINGS
N/A
Case description
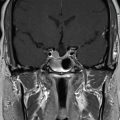
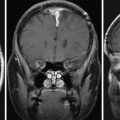
The patient is a 47-year-old female who presented with decreased left visual acuity. The neuroophthalmological examination revealed a dramatic deficit with only 20% residual vision. Magnetic resonance imaging (MRI) showed mirror cavernous sinus meningiomas, where the left symptomatic meningioma is exceptionally large with infratemporal extension and invasion of the optic foramen and superior orbital fissure ( Figure 5.23.1 ). Planned subtotal resection was performed, and the patient completely recovered left eye vision postoperatively. A fat graft was placed intraoperatively between the residual tumor and left optic nerve to facilitate subsequent stereotactic radiosurgery (SRS) (see Figure 5.23.1 ). Postoperative MRI revealed residual left intracavernous sinus meningioma ( Figure 5.23.1 ). Gamma Knife radiosurgery (GKRS) followed as planned ( Figure 5.23.2 ).
Radiosurgery Machine
Gamma Knife – Icon
Radiosurgery Dose (Gy)
14, at the 50% isodose line
Biologically Effective Dose (Gy)
7.7 Gy
Number of Fractions
1
Figure 5.23.1.
Coronal T1-gadolinium injected MRI before surgery (left), immediately after surgery showing the residual tumor (right), and an intraoperative image of fat graft placement between the residual tumor and optic pathways (lower). This maneuver allows delivery of therapeutic radiation doses while avoiding potential radiation-induced optic neuropathy from a single session/fraction stereotactic radiosurgery (SRS) in case of intimate contact between the lesion and optic apparatus. Without spacing the tumor from the optic apparatus, hypofractionated radiosurgery (as opposed to single session) would have been indicated to decrease the risk of optic neuropathy.
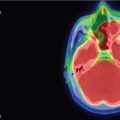
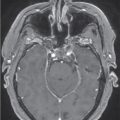
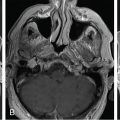
Figure 5.23.2.
Upper panel, left: coronal T2 TSE (green is the 8-Gy isodose line, corresponding to the maximal dose received by the optic apparatus; left optic nerve is colored in magenta); and right: axial T1 gadolinium injected. Lower panel, left: coronal T1-gadolinium injected; and right: axial fat-saturation sequence. Dosimetry is colored in yellow and corresponds to the 14-Gy dose prescription. The left optic nerve (in magenta) received less than 8 Gy. TSE, Turbo-spin-echo.
Critical Structure
Dose Tolerance
Optic pathways
The maximal dose to the optic pathways in patients without prior radiotherapy was classically 8 Gy
Recently, the dose limit has been extended to 10 or even 12 Gy
Cavernous internal carotid artery (ICA)
New or progressive ICA stenosis/occlusion after stereotactic radiosurgery for cavernous sinus meningiomas (CSMs) is considered common by some authors
ICA encasement or constriction increases the risk of ICA stenosis/occlusion, but the risk of ischemic complications is very low
Cavernous sinus neural contents
Cranial nerves within the cavernous sinus are more radioresistant compared to the optic nerve; however, they are considered more sensitive in case of prior irradiation
Only gold members can continue reading. Log In or Register to continue
Apr 6, 2024 | Posted by drzezo in GENERAL RADIOLOGY | Comments Off on Cavernous sinus meningioma – immediate postoperative radiosurgery for perioptic residual


 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
 Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
 Capillary hemangioma – postoperative radiosurgery for residual tumor
Capillary hemangioma – postoperative radiosurgery for residual tumor
 Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual



