Central Nervous System Tumor Mimics
Overview
Nonneoplastic intracranial mass lesions that mimic brain tumors can be difficult to differentiate from true brain tumors based on clinical, laboratory, or imaging findings. Accurate preoperative differentiation between the two entities is essential for proper surgical and medical management of patients presenting with intracranial mass.
Central nervous system (CNS) tumor mimics fall into three general categories of disease process: infectious, inflammatory, and ischemic/vascular diseases. It is important to consider one of these entities as a possible diagnosis when an apparent brain tumor is suspected on imaging because both entities can look alike and radical surgical resection of a brain tumor mimic can potentially lead to a devastating outcome for the patient.
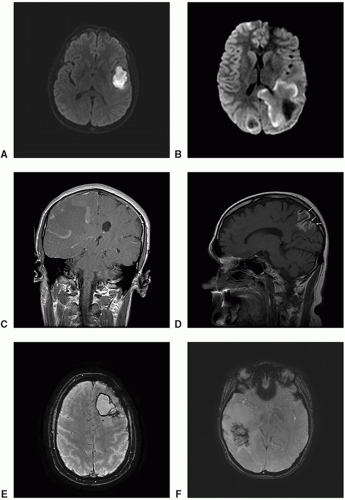 Figure 20.1. Six MR imaging features to identify brain tumor mimics. A. Axial DWI: Homogeneously reduced diffusion within a pyogenic abscess. B. Axial diffusion-weighted imaging (DWI): Peripheral incomplete rim of reduced diffusion of demyelinating lesions. C. Axial T1-postcontrast: Incomplete rim of enhancement of demyelinating lesion. D. Sagittal T1-precontrast imaging: Gyral form of T1 shortening in a subacute infarct. E. Axial T2: Thin complete rim of T2 shortening in a cavernous malformation. F. Axial SWI: Parallel stacked pattern of thrombosed vein in a region of venulitis. |
Central Nervous System Infections
Central nervous system (CNS) infections are caused by various microbes, including but not limited to bacteria, viruses, fungi, parasites, protozoans, or prions, and manifested as meningitis, encephalitis/cerebritis, empyema, or brain abscess. The clinical signs and symptoms of CNS infection are often nonspecific and include headache, fever, altered mental status, and behavioral changes. A high index of suspicion, prompt diagnosis, and therapy of CNS infection are of utmost importance, which can positively impact clinical course and outcome. Delay in diagnosis and treatment of CNS infection, especially in cases of bacterial meningitis or herpes encephalitis, can lead to serious complications and negative outcomes.
Pyogenic abscesses of the brain are thought to result from a bacterial seeding of already devitalized tissue. Brain abscess can mimic malignant brain tumor but each requires vastly different urgent and long-term treatment. Neuroimaging of the two entities can appear very similar as well, but there are a few imaging findings that can help to distinguish brain abscess from the brain tumor. Homogeneously reduced diffusion or incomplete rim of reduced diffusion within a rim-enhancing mass suggests brain abscess although it is not definitive enough to exclude brain tumor. Neuroimaging findings need to be correlated with laboratory findings, especially cerebrospinal fluid (CSF) and white blood cell counts, as well as high index of suspicion for prompt and accurate diagnosis of CNS infection.
 Figure 20.2. Imaging of CNS Infection, nocardia pyogenic abscess. A. Axial T1-precontrast: Large heterogeneously mixed intensity bi-lobed mass in the left parietal lobe. B. Axial fluid-attenuated inversion recovery (FLAIR): Heterogeneously mixed intensity mass with marked surrounding vasogenic edema. |
 Figure 20.2. (continued) C. Axial susceptibility-weighted imaging (SWI): Nodular blood products within the anterior component. D-F. Sagittal T2: Multiple loculated collections in the left parietal lobe with severe surrounding vasogenic edema. G-I. Sagittal T1-postcontrast: Thick rim and nodular rim enhancement of the loculated collections. |
 Figure 20.2. (continued) J-L. Axial DWI: Marked reduced diffusion within several dominant loculated pyogenic collections. M-O. Axial apparent diffusion coefficient (ADC): Marked reduced diffusion within several dominant loculated pyogenic collections. |
 Figure 20.2. (continued) P-R. Axial T1-postcontrast: Thick rim and nodular rim enhancement of the loculated collections. |
 Figure 20.3. Imaging of CNS infection, tuberculoma. A-C. Axial T2: Subtly out-lined hypointense mass in the left thalamus and midbrain with marked surrounding edema. D-F. Axial (D), coronal (E), sagittal (F) FLAIR: Hypointense mass in the left thalamus and midbrain is bettered delineated (black arrows). |
 Figure 20.3. (continued) G-I. Axial DWI: Subtle incomplete rim (white arrows) of reduced diffusion. J-L. Axial T1-postcontrast: Avid and homogeneous enhancement within the mass. |
 Figure 20.4. Imaging of CNS infection, neurocysticercosis. A-C. Axial T1-precontrast: Tri-lobed hypointense mass with subtle rim of T1 shortening (arrows). D-F. Coronal FLAIR: Homogeneously hypointense mass with marked surrounding edema. |
 Figure 20.4. (continued) G-I. Axial DWI: Homogeneously hypointense mass with rim of reduced diffusion (black arrows). J-L. Axial ADC: Homogeneously hyperintense mass with rim of reduced diffusion. |
 Figure 20.4. (continued) M-O. Axial T1-postcontrast: Thin rim of enhancement of the tri-lobed mass. |
Central Nervous System Inflammatory (Noninfectious) Disease
Primary, noninfectious, neuroinflammatory disorders of the CNS are a heterogeneous group of diseases with varying causes and manifestations that include but are not limited to multiple sclerosis, tumefactive demyelinating disease, neuromyelitis optica, acute disseminated encephalomyelitis, primary angiitis, autoimmune limbic encephalitis, Susac’s syndrome, neurosarcoidosis, systemic lupus erythematosus, giant cell arteritis, Behçet’s disease, Sjögren’s syndrome, and other vasculitides. During the acute inflammatory phase, CNS inflammatory disorders can present as mass lesions mimicking aggressive brain tumor with enhancement, hemorrhage, mass effect, and/or surrounding edema. It is
essential to consider CNS inflammatory diseases in the differential diagnosis of any brain masses, especially those with one or more of the six imaging characteristics listed in Table 20.1.
essential to consider CNS inflammatory diseases in the differential diagnosis of any brain masses, especially those with one or more of the six imaging characteristics listed in Table 20.1.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


