Cerebrospinal Fluid Disorders
Obstructive Hydrocephalus, Intraventricular
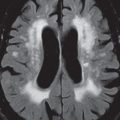
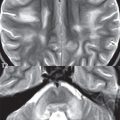
This entity is defined by obstruction proximal to the foramina of Luschka and Magendie. It can be acute or chronic (compensated) ( Fig. 1.144 ). The ventricular system proximal to the level of obstruction will be dilated, with the dilated portion more round in appearance (“ballooned”). In cases of acute obstruction there will also be abnormal high signal intensity on T2-weighted scans in the periventricular white matter (best seen on FLAIR, as a thick smooth hyperintense rim), representing interstitial edema. The sulci and cisterns will be effaced, and the corpus callosum thinned: the latter in cases where the lateral ventricles are both enlarged.

Obstructive Hydrocephalus, Extraventricular
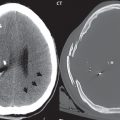
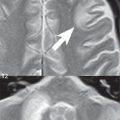
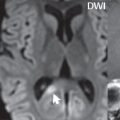
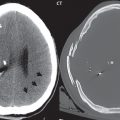
In this entity, also known as communicating hydrocephalus, there is obstruction distal to the outlet foramina of the fourth ventricle. The lateral and third ventricles, and in most cases the fourth ventricle, will be enlarged without evidence of a specific (proximal) lesion causing obstruction. The enlargement of the ventricular system will be out of proportion to any enlargement of the subarachnoid space, the latter as assessed by prominence of the cortical sulci and the sylvian fissures. In some patients the fourth ventricle may appear near normal in size. Important differential diagnostic considerations include ventricular enlargement due to parenchymal atrophy and normal pressure hydrocephalus. The most common cause of extraventricular obstructive hydrocephalus is subarachnoid hemorrhage ( Fig. 1.145 ). Other etiologies include obstruction due to inflammatory or neoplastic exudates, and in this instance leptomeningeal enhancement will be demonstrated on contrast-enhanced MR.

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


