CERVICAL ESOPHAGUS: DEVELOPMENTAL ABNORMALITIES
KEY POINTS
- Imaging may make a precise diagnosis developmental anomalies of the cervical esophagus.
- Imaging will often significantly affect medical decision making in these developmental conditions.
- Computed tomography and/or magnetic resonance imaging are typically the main and frequently the only studies required.
- Ultrasound usually will not provide information definitive enough for medical decision making.
Some developmental conditions present as masses or because they interfere with function. In the cervical esophagus, they may manifest as dysphagia or odynophagia; the latter two symptoms might be present with poor feeding in an infant (Fig. 222.1) or symptoms of associated anomalies (Figs. 222.2–222.6). They are typically not painful unless there is some complicating factor. Developmental abnormalities may also manifest because of such complicating factors. Examples include infection in an esophageal or foregut duplication cyst that connects to the cervical esophagus (Fig. 222.3) or pharynx as well as bleeding, thrombosis, or infection of a vascular malformation. Developmental abnormalities may also be discovered incidentally on imaging studies done for other purposes (Fig. 222.5).
The natural history and imaging appearance of the rare developmental cysts are discussed in Chapter 8. Vascular malformations may secondarily involve the cervical esophagus (Chapter 9). A tracheoesophageal fistula is likely to be part of a syndrome or at least seen in the presence of other anomalies. Other structural abnormalities such as diverticuli at the hypopharyngeal and esophageal junction are considered here since they arise from developmental deficiencies, or at least predispositions, in those muscular walls (Figs. 222.5 and 222.6).
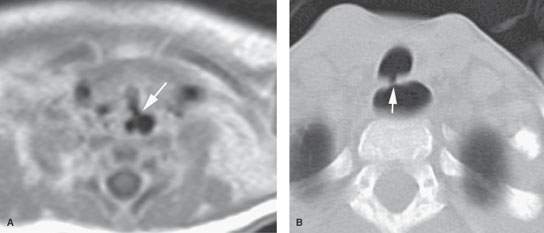
FIGURE 222.1. Two patients with tracheoesophageal fistulas associated with other anomalies. A: An infant with multiple congenital anomalies also demonstrating a tracheoesophageal cleft, as seen on this contrast-enhanced T1-weighted magnetic resonance image. B: A pediatric patient with Goldenhar syndrome. Computed tomography study shows a tracheoesophageal fistula that was not suspected but did finally explain why the patient coughed every time he ate.
ANATOMIC AND DEVELOPMENTAL CONSIDERATIONS
Embryology
The embryology of some of the conditions that affect the foregut are presented in the chapters on laryngeal, hypopharyngeal, and tracheal developmental abnormalities (Chapters 202, 210, and 216). It is useful to also understand the branchial apparatus development, including its thymic and parathyroid components, presented in Chapter 153 (Fig. 222.4).
Hypopharyngeal–cervical esophageal diverticuli are more likely to be lateral (Fig. 222.5) than midline posterior on a congenital basis but really must, at least in childhood, be considered in this category of a developmental disorder.
Applied Anatomy
A thorough knowledge of esophageal anatomy and anatomic variations is required for the evaluation of developmental conditions of the esophagus. This anatomy is presented in detail with the introductory material on the esophagus (Chapter 221), hypopharynx and larynx (Chapters 201 and 215), and related spaces of the neck (Chapters 142 and 149).
IMAGING APPROACH
Techniques and Relevant Aspects
The esophagus is studied in essentially the same manner for developmental abnormalities and benign masses of known or uncertain etiology as it is for the evaluation of known or suspected esophageal cancer. Such studies should be continued to the carina. The principles of using these studies for the esophagus in general are reviewed in Chapter 221. Specific problem-driven protocols for computed tomography (CT) and magnetic resonance imaging (MRI) of the esophagus are presented in Appendixes A and B, respectively.
There is little or no use for ultrasound in studying these conditions except for the in utero evaluation of fetal swallowing and intraluminal ultrasound, which are beyond the scope of this text.
Pros and Cons
In general, these occur in younger age groups, so it is best to avoid radiation if possible. On the other hand, definitive MRI in children may require general anesthesia. These relative risks must be balanced. Either MRI or CT is usually definitive in the anatomic evaluation of these anomalies of development. One or the other may be more specific in some circumstances. MRI is more likely to be motion degraded, which may be particularly relevant when imaging small children.
Potentially developmental lesions that present as infections are better evaluated by CT. Such imaging is also more likely to show calcifications, if this is important for the differential diagnosis. MRI provides a better map of venolymphatic malformations and can help to characterize cystic masses with diffusion-weighted imaging.
There really is no generally correct or incorrect choice in this matter. The decision of which imaging study to use should be individualized based on age, likelihood of the correct diagnosis already being known from clinical information, and availability of imaging equipment and other factors just discussed.
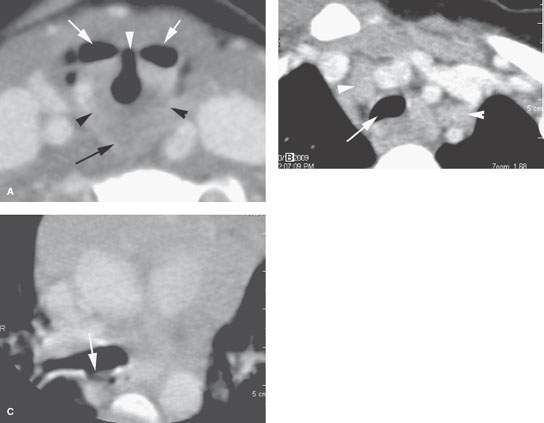
FIGURE 222.2. A 3-year-old patient presenting with sleep apnea and possibly aspiration. This contrast-enhanced computed tomography study shows an atypical arrangement of the supraglottic larynx and pharynx believed to be due to a cleft larynx or at least incomplete partition of the larynx and pharynx during development. In (A), the deformed laryngeal vestibule (arrow) bears an abnormal relationship to the pyriform sinuses (arrowhead). In (B), the abnormally shaped trachea suggests localized tracheomalacia (arrow). In (C), a suggested tracheoesophageal fistula could not be confirmed at endoscopy.
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Hypopharynx: Developmental Abnormalities
Hypopharynx: Developmental Abnormalities
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


