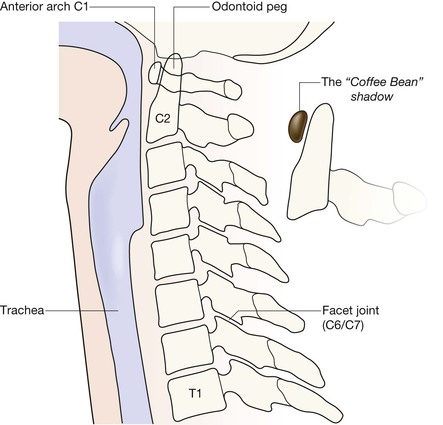
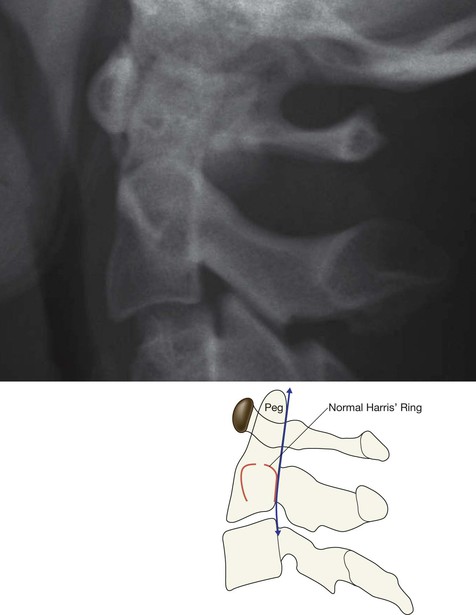
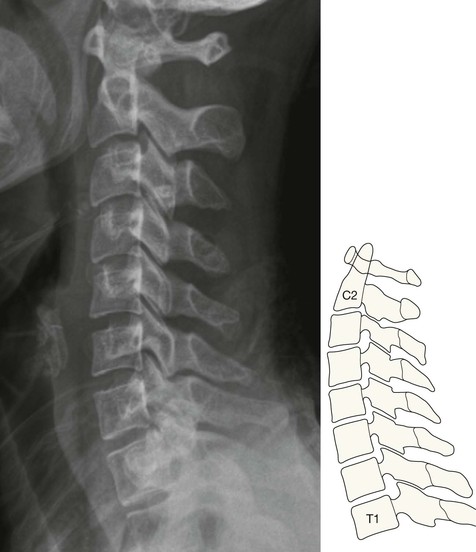
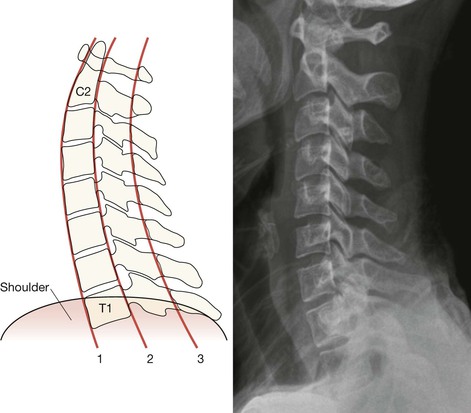
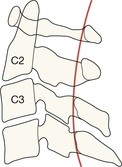
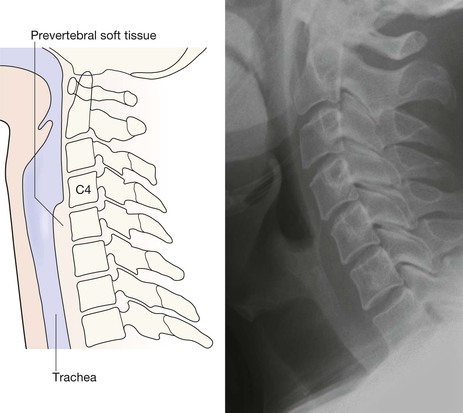
The Coffee Bean Shadow. The anterior arch of C1 is a shadow that is always visible on a lateral radiograph. It looks like a reversed capital D. We call this shadow the “Coffee Bean” shadow because we think it resembles a coffee bean. Use it as your anatomical starting point when assessing the C1–C2 anatomy. Injuries are most often missed because of poor radiographic technique and/or inaccurate film interpretation1,2,4–6. Most errors are avoidable5. Missed C-spine abnormalities occur most commonly at the top or at the bottom of the C-spine1,2. □ Whatever the level of violence, C-spine injuries frequently occur at the C1–C2 level1,3,4,6. □ The most common fracture in elderly patients following a fall is a high cervical injury1,3. □ Between 9% and 26% of patients with one fracture or dislocation of the spine will have further fractures demonstrable radiographically at other levels5. Identify the odontoid peg and assess its position and anatomical relationship to the C1 vertebra. Overlapping structures (eg mastoid, ear lobes, C1 vertebra) can make this difficult. Questions 1–5 will help you to overcome this. 2. Have I identified the anterior arch of the C1 vertebra (the “coffee bean”)? 3. Is the anterior cortex of the odontoid peg (the Peg) closely apposed to the “coffee bean”? 6. Is Harris’ ring7 normal? A break in either the anterior or posterior margin of the ring indicates the high probability of a fracture of the Peg/body of C2 (p. 176). 7. Are the posterior arches of C1 and C2 intact? 8. Are the other vertebrae (C3–C7) intact (p. 192)? 9. Are the three main contour lines/arcs normal (p. 178)? Questions 2 and 3. Recognising the anterior arch of C1 is key to detecting the abnormalities that may involve the C2 vertebra. The arch looks like a small coffee bean, and is always easy to identify on the lateral view. The gap between the Peg and the coffee bean should not exceed 3 mm in adults or 5 mm in children1. This is a normal lateral view. Questions 4 and 5. Check that the anterior cortex of the Peg is continuous with the anterior cortex of the body of C2. Also check that the posterior cortex of the Peg is continuous with the posterior cortex of the body of C2. Any displacement or break in either of these lines indicates a Peg fracture. Question 8. Check that the vertebral bodies (C3–C7) are intact. The vertebral bodies below C2 have a fairly uniform square or rectangular shape. The anterior and posterior heights should be approximately the same. The front to back widths of all of the vertebrae are approximately similar. Question 9. You can trace the three main contour lines (arcs) as follows: Line 1: along the anterior margins of the vertebral bodies (anterior line). Line 2: along the posterior margins of the vertebral bodies (posterior line). Line 3: along the bases of the spinous processes (spinolaminar line). Each line should be a smooth unbroken curve or arc. No kink. No step. Trace these lines along the full length of the cervical spine. Line 1 extends from the top of the anterior cortex of the Peg to the anterior margin of the body of T1 vertebra. Potential Pitfall: Line 3 will sometimes show a slight step at the C2 level, particularly in children8. Apply this rule: this step should not be more than 2 mm posterior to the smooth arc as it is traced upwards between C3 and C1 vertebrae. Question 10. Are the pre-vertebral soft tissue shadows normal? The soft tissue shadow7,9–11 anterior to the vertebral bodies has a characteristic configuration and width. Any bulge or local increase in width indicates haemorrhage and connotes an important injury. NB: The absence of a bulge does not exclude a ligamentous or bone injury. Indeed, even with a major injury, a soft tissue bulge due to a haematoma is fairly rare. The anatomical arrangement of the C1–C2 articulation allows extensive neck rotation whilst providing maximum stability. This stability depends on the integrity of the ligaments, particularly the C2 transverse ligament. Various other ligaments enable C1 vertebra to be held in the optimal position above the body of C2 vertebra. Any deviation from this alignment indicates either ligamentous disruption or a broken vertebra. Ask yourself three important questions:
Cervical spine
Normal anatomy
Lateral view
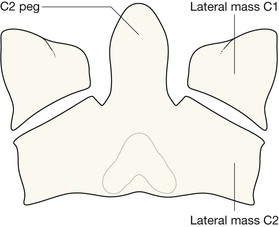
AP Peg view
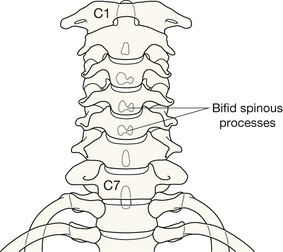
Long AP view
Analysis: the checklists
Priority 1: Lateral view checklist
Ask yourself ten important questions:

Priority 2: AP Peg view checklist
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



Cervical spine
11





