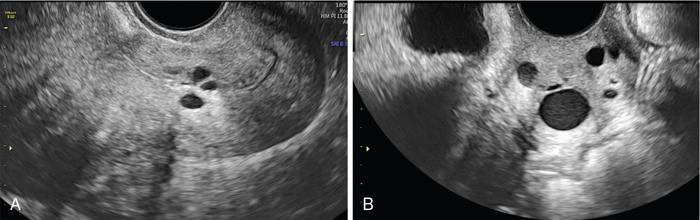
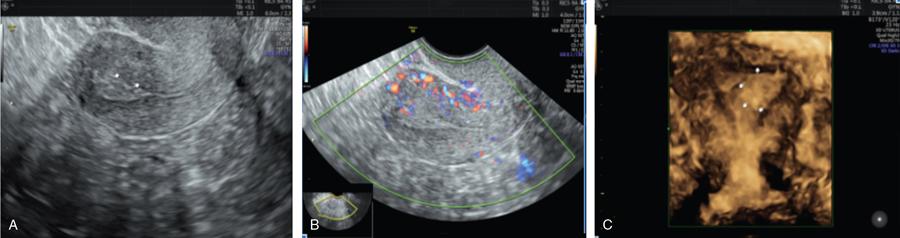
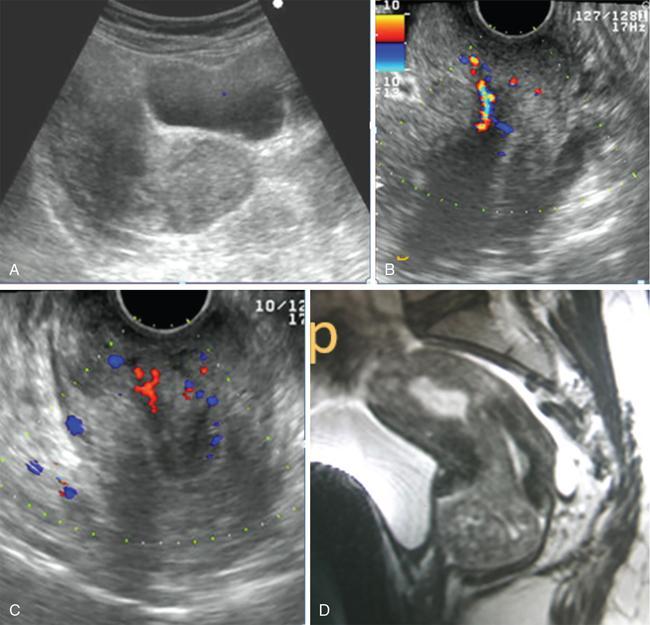
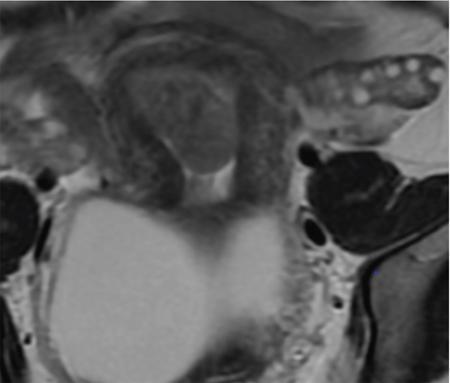
John De Lindsay, Usha Nandini Ganeshan, Vidya CERVICITIS Acute or chronic inflammation of cervix is termed as cervicitis. Noninfectious causes of cervicitis include trauma, pelvic radiation and chemical irritation. Most acute cervicitis is secondary to an infectious agent, commonly Trichomonas vaginalis, Candida albicans, herpes simplex virus, Neisseria gonorrhoeae and Chlamydia trachomatis. Patients usually present with purulent or mucopurulent cervical and vaginal discharge and may complain of pelvic pressure or discomfort. The cervix in patients with acute cervicitis shows a diffusely heterogeneous echotexture of the cervical mucosa and stroma, but the key finding is markedly increased vascularity on colour Doppler. Absence of mass is the differentiating feature between inflammation and malignancy. Free fluid can also be seen in the pouch of Douglas. CT may demonstrate an enlarged uterine cervix, an abnormally enhancing endocervical canal, and parametrial fat stranding. Retention cysts of the uterine cervix are termed as nabothian cysts. They are formed as a result of the healing process of chronic cervicitis. They are usually less than 1 cm, incidentally detected at imaging and are considered a normal finding in multiparous women. They may enlarge and become symptomatic because of mass effect, but this happens infrequently Majority of nabothian cysts, appear as small, simple anechoic cysts in the cervix, with no internal vascularity (Fig. 11.18.1.1). Their appearances can also vary depending upon any internal proteinaceous or haemorrhagic content, cyst clustering and deeper cervical stromal extension. US features that raise concern for malignancy include a solid component and marked vascular flow in the lesion at colour Doppler US. Tunnel cluster is a special variant of nabothian cyst with complex multicystic dilatation of the endocervical glands. Though macroscopically it resembles adenoma malignum, the epithelial cells of the tunnel cluster, do not show any cellular atypia similar to nabothian cyst. Nabothian cysts exhibit intermediate or slightly high signal intensity on T1-weighted (T1W) images and have prominent high signal intensity on T2-weighted (T2W) images. Presence of a solid component surrounding or separating the cysts gives us a clue to differentiate adenoma malignum from a benign nabothian cyst cluster. MR imaging also may be helpful in distinguishing adenoma malignum from benign multicystic lesions of the cervix. MR imaging features associated with malignancy include irregular margins, enhancing solid components, local invasion and metastases. CERVICAL STENOSIS Stenosis of the uterine cervix is the pathological narrowing of the cervix. The term cervical stenosis is clinically defined as cervical narrowing that prevents the insertion of a 2.5-mm-wide dilator. In utero exposure to diethylstilbestrol contributes about 20% of the cases. Often associated with endometriosis. Cervical stenosis in menopausal patient is asymptomatic. Retrograde menses may occur in women of reproductive age, thus posing a risk of endometriosis. Dysmenorrhea is present in up to 50% of patients with cervical stenosis. If the stenosis is severe enough, it may result in proximal obstruction resulting in haematometra, hydrometra, pyometra, haematosalpinges. The symptoms depend upon the severity of stenosis. Other potential consequences include infertility, impediment to assisted fertility techniques – embryo transfer and intrauterine insemination. Any pathological process that can cause inflammation of the cervical mucosa, resulting in erosion and regeneration can result in cervical stenosis. This includes: Narrowing of the endocervical canal may be observed (normal diameter: 0.5–3.0 cm). Complete obliteration of the cervical os will prevent insertion of the hysterosalpingographic catheter. The endocervix can be normal in appearance or slightly thickened. If post irradiation, the cervix may demonstrate loss of the normal zonal architecture. There may be mild to moderate fluid distension of the endometrial cavity (Fig. 11.18.2.1). If the fluid has internal echoes a careful search for potentially associated endometrial or cervical mass lesions, should be done. Complex, particulate intracavitatory fluid with its heterogeneous echogenicity at ultrasound may mimic a solid lesion; however, the absence of detectable flow at colour Doppler US and the central location should suggest the correct diagnosis. May reveal complications due to cervical stenosis such as hydrometra and haematometra and haematosalpinges. Though the cervix may be appear normal, the uterine cavity may be fluid filled. Auxiliary findings may suggest an underlying cause, such as an obstructive mass lesion, or post radiation bowel wall thickening. In equivocal cases, MR imaging may be useful to differentiate complex endocervical fluid from a mass. In selected situations, gradual dilatation of the cervix under ultrasound guidance, can be an effective treatment. Depending on severity of disease, other treatment options include insertion of laminaria tent, hysteroscopic cervical excision or in extreme cases total hysterectomy. CERVICAL POLYPS The common cervical polyps are prolapsing endometrial polyps. They are seen in endocervial canal. Endometrial polyps are common and a frequent cause of abnormal uterine bleeding. They account for approximately 30% of cases of postmenopausal bleeding. In menstruating females, they may cause intermenstrual bleeding, metrorrhagia, and infertility. Polyps can be histologically characterized as localized hyperplastic overgrowths of glands and stroma covered by epithelium. The typical appearance of an endometrial polyp at sonography is a well-defined, homogeneous, polypoid lesion that is isoechoic to hyperechoic to the endometrium with preservation of the endomyometrial interface (Fig. 11.18.3.1). There usually is a well-defined vascular pedicle within the stalk demonstrated on colour Doppler sonography (Fig. 11.18.3.2). Uncommon features of polyps include multiplicity, cystic components, a broad base and hypoechogenicity or heterogeneity. Occasionally, polyps can have a heterogeneous echotexture with multiple cysts. This complex appearance may be due to haemorrhage, infarction or inflammation within the polyp. Sonohysterography is an ultrasound technique in which the endometrial cavity is distended with saline allows evaluation of single layer of the endometrial lining and enables us to reliably distinguish focal from diffuse endometrial pathologic conditions. Focal lesions are defined as lesions occupying less than 25% of the endometrial surface area and diffuse lesions involve a larger percentage of the endometrial surface area. Saline infusion sonohysterography which involves the infusion of fluid to visualize the endometrium is a simple, well-tolerated and inexpensive procedure. Sonohysterography is best performed as soon as possible after the bleeding cycle has ended when the endometrium is thin. When the patient has irregular bleeding, that she cannot tell what is actual menses, in such cases it may be helpful to use an empiric course of a progestogen such as medroxyprogesterone acetate 10 mg daily for 10 days as a medical curettage and then time the ultrasound examination to the withdrawal bleed. The decision about whether to obtain cultures and use of antibiotics depends very much on the patient population with which the physician deals with. Anaesthesia or analgesia is not required. A bimanual examination to know the version of the uterus is done. The vaginal speculum is inserted. Under sterile aseptic precautions, a catheter is inserted into the cervix. This is done by grasping the cervix with a ring forceps feeding it through the os. A cervical stabilizer may be used and it will be less painful, less traumatic and does not cause bleeding from the cervix. The speculum is removed without dislodging the catheter. The vaginal probe is then reinserted. A 10-mL syringe is attached to catheter. Scanning in long-axis projection, fluid is instilled while watching the video monitor. In that long-axis projection the transducer is removed from side to side (i.e. from cornua to cornua). The amount of fluid instilled is variable and depends on the image which is producing on the ultrasound screen. When the uterus has been completely rotated 90 degrees into a coronal plane further fluid is instilled, while fanning down toward the endocervical canal and up toward the uterine fundus. Very minimal fluid acts as a sufficient interface to distinguish anterior and posterior endometrial surfaces and outline endometrial pathology. The risk of malignant cell dissemination exists but is small. The saline infusion sonohysterography can reliably distinguish dysfunctional abnormal bleeding (no anatomic abnormality) from those with globally thickened endometrium. Endometrial polyp appears as homogeneous, well-circumscribed, polypoid lesion that is isoechoic to the endometrium with preservation of endometrial–myometrial interface. Other features can be cystic components, multiplicity, a broad base, and hypoechogenicity or heterogeneity. Submucosal leiomyomas are usually broad-based, hypoechoic, well-defined, solid masses with shadowing and an overlying layer of echogenic endometrium that distorts the endometrial–myometrial interface. They are pedunculated or have a multilobulated surface. The major advantage of sonohysterography is the accuracy in depicting the percentage of the fibroid that projects into the endometrial cavity. In contrast to the transvaginal US demonstration of polyps, which may distort measurements of endometrial thickness if made before saline infusion, at sonohysterography the uninvolved single-layer endometrium appears normal in thickness and should be measured separately from the polyp. The findings at sonohysterography determine whether a blind biopsy, hysteroscopically guided biopsy, or hysteroscopically guided dilation and curettage is the appropriate diagnostic. On MRI polyps appear T2 isointense to hypointense and demonstrate postcontrast enhancement (Fig. 11.18.3.3). Polyps generally enhance less than the surrounding endometrium but more than myometrium. Most of endometrial polyps can be reliably differentiated from submucosal leiomyomas on MR imaging with leiomyomas having hypointense signal on T2W and visualizing origin from the myometrium. A small percentage of endometrial polyps may contain malignant foci or foci of endometrial hyperplasia. Hormones (endogenous or exogenous), tamoxifen usage, nulliparity, obesity, hypertension and diabetes. Histologic patterns of endometrial hyperplasia vary from hyperplasia without atypia, which has little or no malignant potential, to severe atypia in which 20% of cases progress to endometrial cancer. Endometrial hyperplasia accounts for approximately 4%–8% of cases of postmenopausal bleeding. In sonohysterography, endometrial hyperplasia appears as a diffuse thickening of echogenic endometrial stripe without focal abnormality, uncommonly focal endometrial hyperplasia can be seen. In sonohysterography the latter form of hyperplasia is more difficult to differentiate from endometrial polyps because characteristics of the focal endometrial thickening in both conditions overlap. Endometrial cancer is typically a diffuse process, but early cases can appear as a polypoid mass. Imaging features of endometrial hyperplasia include irregular thickening of the endometrium with T2 hyperintensity compared to normal myometrium and T1 hypointensity relative to myometrium on early contrast-enhanced images. Endometrial thickening measuring >5 mm in postmenopausal females with bleeding, regardless of hormonal therapy should undergo further investigation including tissue sampling to exclude endometrial cancer. Cervical polyps are the commonest causes of intermenstrual vaginal bleeding. Most patients are perimenopausal present with symptoms including menorrhagia, postmenopausal bleeding, contact bleeding and vaginal discharge. Pathologic conditions of cervical polypoid lesions include endometrial or endocervical tissue with metaplasia, leiomyoma, inflammation or malignancy or even blood clot. Most common are endocervical polyp, account for more than 60% of cervical polypoid lesions. More commonly polyps are pedunculated, with a slender pedicle of varying length, but few are sessile. The diagnosis is made primarily with hysteroscopy. Endocervical polyps are usually seen as masses with or without cysts filling endocervical or vaginal canal. Identifying the stalk attaching to the cervical wall may differentiate it from endometrial polyp. On USG it appears hypoechoic or echogenic with a stalk. CERVICAL CARCINOMA Cervical carcinoma is the third most common gynaecological malignancy after endometrial and ovarian malignancies. It affects middle-aged females from 35 to 50 years with an average age of onset at around 45 years. It is one of the leading causes of deaths among women in developing countries. Prognosis depends on tumour size, nodal status, histological grading and staging at the time of diagnosis. So accurate staging of the disease is very important to decide the treatment strategy.
11.18: Cervix
Ultrasound
CT
Nabothian cysts
Ultrasound
MR imaging
Introduction
Epidemiology
Clinical presentation
Pathology
Aetiology
Radiological features
Hysterosalpingogram
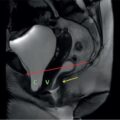
Ultrasound

CT
MR
Treatment and prognosis
Differential diagnosis
Saline infusion sonography
Endometrial hyperplasia
Cervical polyps
Introduction
Risk factors
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


