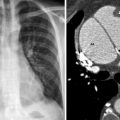
Fig. 38.1
Chest radiograph demonstrates typical findings associated with aortic injury: downward displacement of the left mainstem bronchus (a), right sided displacement of the esophagus with nasogastric tube shifted to the right of midline (b), widened superior mediastinum and ill-defined aortic knob (c), trachea and endotracheal tube shifted to the right of midline (d)
Table 38.1
Plain chest film features associated with aortic injury
Widened mediastinum |
Prominent or obliterated aortic knob |
Trachea deviated to the right |
Esophagus deviated to the right |
Left main bronchus depression |
Hemothorax |
Loss of aorto-pulmonary window |
Left apical cap |
CT imaging is the reference standard for diagnosing aortic injury (Figs. 38.2 and 38.3). With modern scanners and higher resolution output, the sensitivity and negative predictive value of CT in evaluating the integrity of the thoracic aorta approaches 100 %. Further, the wide availability, speed, safety, and ease of interpretation make CT more attractive than formal angiography. The CT findings associated with aortic injury are summarized in Table 38.2. Despite the numerous strengths of the CT in evaluating aortic injuries, its sensitivity and specificity can vary among centers and radiologists. Potential pitfalls in imaging the thoracic aorta, including failure to distinguish true intimal injuries from anatomic variants—such as ductus diverticulum—and pulsation artifact, are minimized with experienced image interpretation.
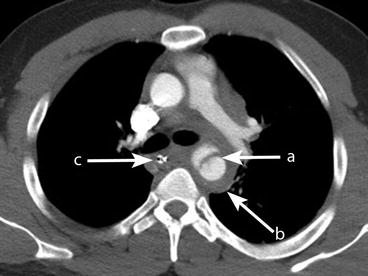

Fig. 38.2
Multi-detector computed tomography (CT) angiogram demonstrating: pseudoaneurysm distal to the aortic isthmus (a), surrounding mediastinal hemorrhage (b), rightward displacement of the esophagus (c)
Fig. 38.3
Sagittal Maximum Intensity Projection (MIP) image demonstrates pseudoaneurysm and intima injury, just distal to the aortic isthmus at the level of the ligamentum arteriosum (a)
Table 38.2




CT features associated with aortic injury
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
