KEY FACTS
Terminology
- •
Malignancy arising from intrahepatic bile duct (IHBD) or extrahepatic bile duct epithelium
Imaging
- •
Best diagnostic clue: Intra- or extrahepatic bile duct mass with upstream bile duct dilatation
- •
Intrahepatic cholangiocarcinoma
- ○
Mass with ill-defined margin, heterogeneous echotexture
- ○
Arise distal to 2nd-order bile ducts
- ○
Isolated thickening of IHBD or intraductal mass with upstream ductal dilatation
- ○
May see associated capsular retraction of liver
- ○
- •
Hilar cholangiocarcinoma
- ○
Dilatation of IHBDs without extrahepatic ductal dilatation
- ○
Nonunion of right and left hepatic ducts due to obstructing mass
- ○
Primary tumor may not be discernible or appears as small, infiltrative iso-/hyperechoic mass in hilar region
- ○
Nodular or polypoid mass in bile ducts
- ○
- •
Extrahepatic cholangiocarcinoma
- ○
Proportional bile duct dilatation
- –
Primary tumor often undetectable due to deep location
- –
- ○
Ill-defined, solid, heterogeneous mass within or surrounding duct at point of obstruction
- ○
Exophytic heterogeneous mass from bile duct
- ○
Polypoidal intraluminal tumor visible as iso-/hyperechoic mass within bile duct
- ○
Top Differential Diagnoses
- •
Pancreatic head adenocarcinoma
- •
Choledocholithiasis
- •
Recurrent pyogenic cholangitis
- •
Primary sclerosing cholangitis
- •
Porta hepatis tumor
Pathology
- •
Pathogenesis: Biliary intraepithelial neoplasm is considered premalignant lesion
Diagnostic Checklist
- •
Rule out other pancreatobiliary pathology causing biliary obstruction
- •
Long focal extrahepatic biliary stricture, irregular ductal wall, stenosis, and prestenotic biliary ductal dilatation
Scanning Tips
- •
Look for capsular retraction, biliary ductal dilatation, or abrupt cut-off of dilated bile ducts
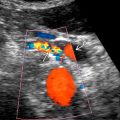
 at the confluence of the right and left hepatic ducts (Klatskin tumor). The mass invades adjacent liver parenchyma and hepatic veins
at the confluence of the right and left hepatic ducts (Klatskin tumor). The mass invades adjacent liver parenchyma and hepatic veins  , a common finding with cholangiocarcinoma. Note upstream dilatation of intrahepatic bile ducts
, a common finding with cholangiocarcinoma. Note upstream dilatation of intrahepatic bile ducts  .
.Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


