Fig. 12.1
Schematic diagram of morphologic classification of bile duct dilatation. (a) In distal obstruction with malignancy or benign stricture, dilatation of whole upstream biliary tree shows proportionate nature, in which large ducts are more dilated than small ducts are. (b) In recurrent pyogenic cholangitis, dilatation of extrahepatic duct and central intrahepatic duct, ductal rigidity and straightening, increased or right-angle branching pattern, decrease in arborization, and acute tapering of peripheral duct are seen. Obliteration of peripheral intrahepatic ducts shows pruned tree appearance. (c) In clonorchiasis, uniform, disproportionate dilatation of biliary tree from the central duct to the far peripheral ducts without extrahepatic duct dilatation. (d) In primary sclerosing cholangitis, multiple segmental strictures involving both the intrahepatic and the extrahepatic bile ducts are seen, with alternating strictures and dilatations produce the “beaded” appearance. Obliteration of peripheral intrahepatic ducts shows pruned tree appearance
12.7.2 Primary Sclerosing Cholangitis
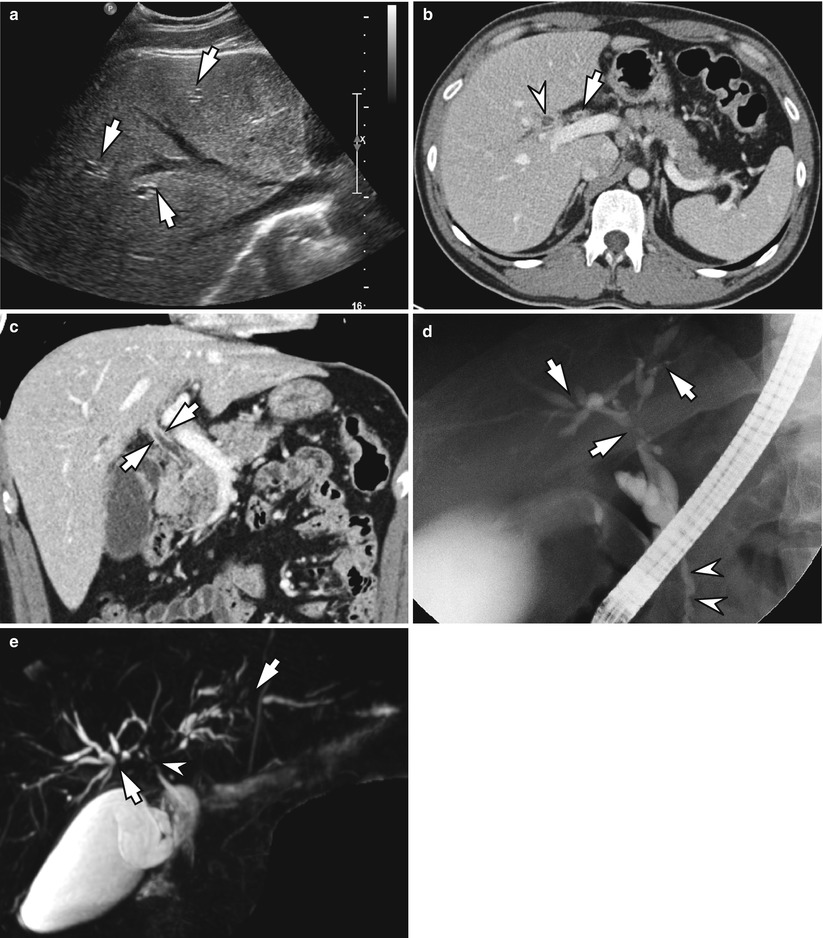
Fig. 12.2
Primary sclerosing cholangitis in a 42-year-old man. (a) Ultrasound shows mild intrahepatic duct dilatation. (b) Axial image of portal phase CT shows mild enhanced wall thickening of common hepatic duct (arrow) and proximal intrahepatic duct (arrowhead). (c). Coronal image of portal phase CT shows diffuse enhanced wall thickening of common duct (arrows). (d) Cholangiography obtained from endoscopic retrograde cholangiography (ERC) shows multifocal strictures and dilatations of intrahepatic ducts (arrows) and multifocal narrowings of common bile duct (arrowheads).(e) Magnetic resonance cholangiopancreatography (MRCP) shows multiple strictures of intrahepatic ducts (arrows) and common hepatic duct (arrowhead)
12.7.3 Primary Sclerosing Cholangitis
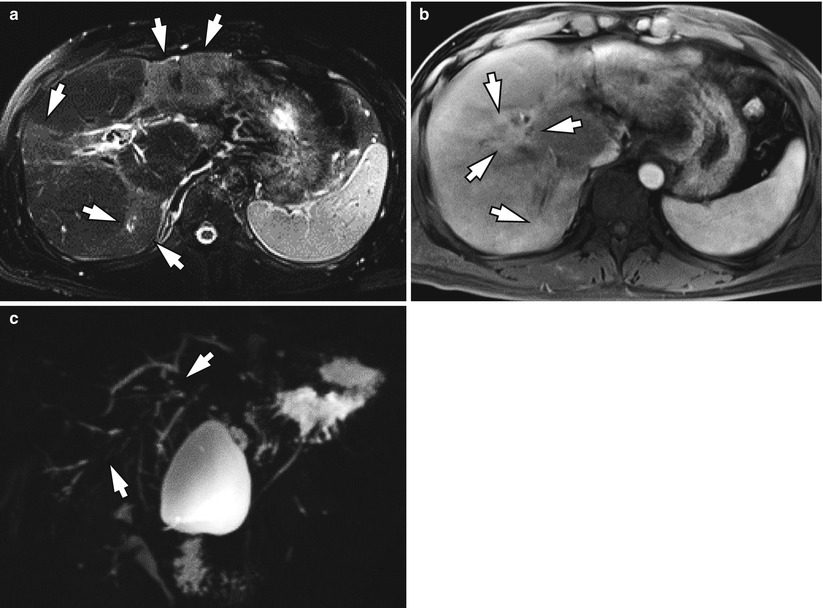
Fig. 12.3
Primary sclerosing cholangitis in a 45-year-old man. (a). Fat-suppressed T2-weighted MR image shows multifocal patchy high signal intensity areas of hepatic parenchyma (arrows). (b) Arterial phase dynamic MR image shows multifocal periductal patchy enhancement (arrows) suggesting cholangiohepatitis. (c) MRCP shows multifocal strictures of intrahepatic ducts with minimal upstream ductal dilatation (arrows). Note the paucity of biliary trees suggestive of pruned tree appearance
12.7.4 Primary Sclerosing Cholangitis
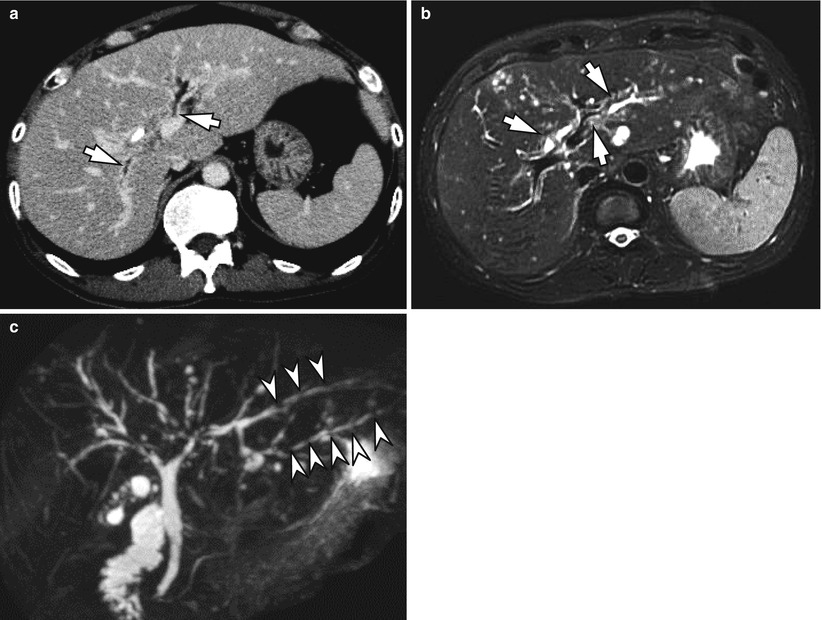
Fig. 12.4
Primary sclerosing cholangitis in a 52-year-old man. (a) Portal phase CT shows enhanced wall thickening with mild dilatation of intrahepatic ducts (arrows). (b) Fat-suppressed T2-weighted MR shows periductal high signal intensities with mild dilatation of intrahepatic ducts (arrows). (c) MRCP shows multifocal strictures with dilatation of intrahepatic ducts with beaded appearance (arrowheads)
12.7.5 Primary Biliary Cirrhosis
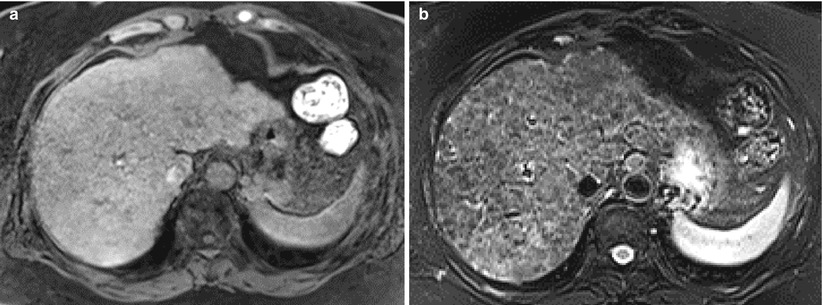
Fig. 12.5
Primary biliary cirrhosis in a 62-year-old woman. (a). Fat-suppressed T1-weighted image shows numerous hepatic nodules intercalated by low signal intensity lacelike fibrosis. (b) Fat-suppressed T2-weighted image shows regenerated nodules as low signal intensity and intercalating fibrosis as high signal intensity (By the courtesy of Prof. Jin Young Choi, Yonsei University College of Medicine)
12.7.6 Hepatolithiasis
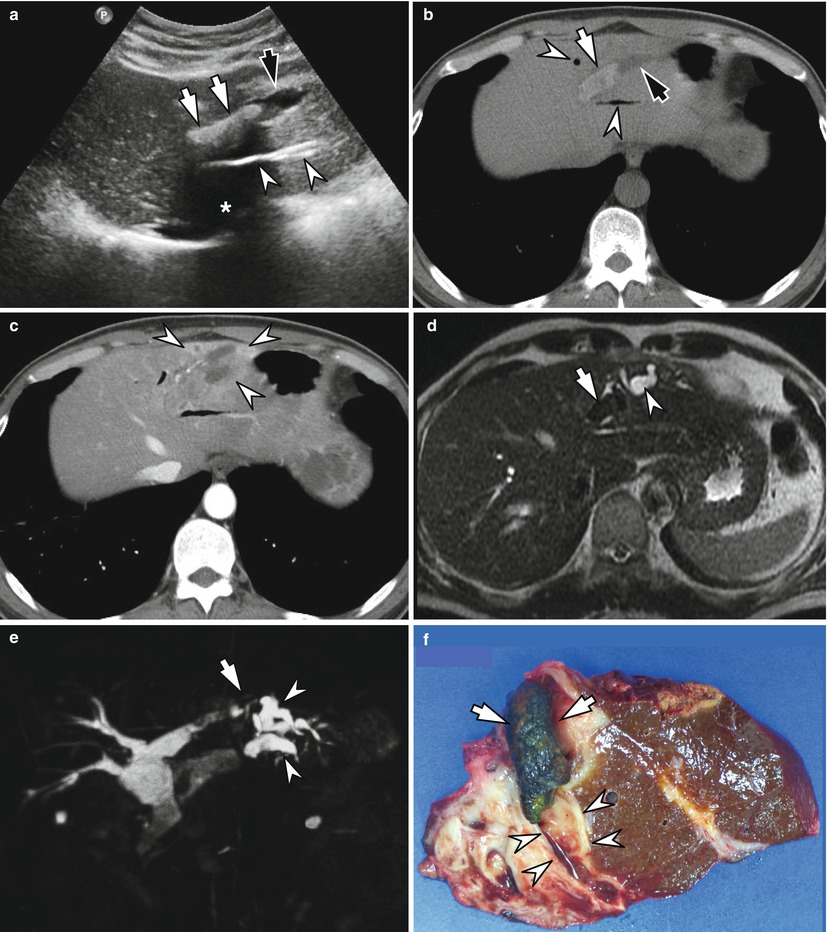
Fig. 12.6
Hepatolithiasis in a 57-year-old man. (a) Ultrasound image shows elongated echogenic material (white arrows) having posterior acoustic shadowing (asterisk) in the left lateral intrahepatic duct with upstream ductal dilatation (black arrow). Air biliary gram is seen as linear strong high echogenic line (arrowheads). (b) Noncontrast CT shows high-density stone in the left lateral intrahepatic duct (white arrow) with upstream ductal dilatation (black arrow). Also note air biliary grams in the neighboring ducts (arrowheads). (c) Arterial phase CT shows patchy periductal enhancement of hepatic parenchyma around intrahepatic duct stone (arrowheads). (d). T2-weighted MR shows intrahepatic duct stone as dark signal intensity (arrow) with upstream ductal dilatation as bright signal intensity (arrowhead). (e) MRCP shows intrahepatic duct stone as signal void (arrow) with upstream ductal dilatations (arrowheads). (f) Gross specimen of left lateral hepatic sectionectomy shows greenish intrahepatic duct stone (arrows) with upstream ductal thickening and dilatation (arrowheads)
12.7.7 Recurrent Pyogenic Cholangitis
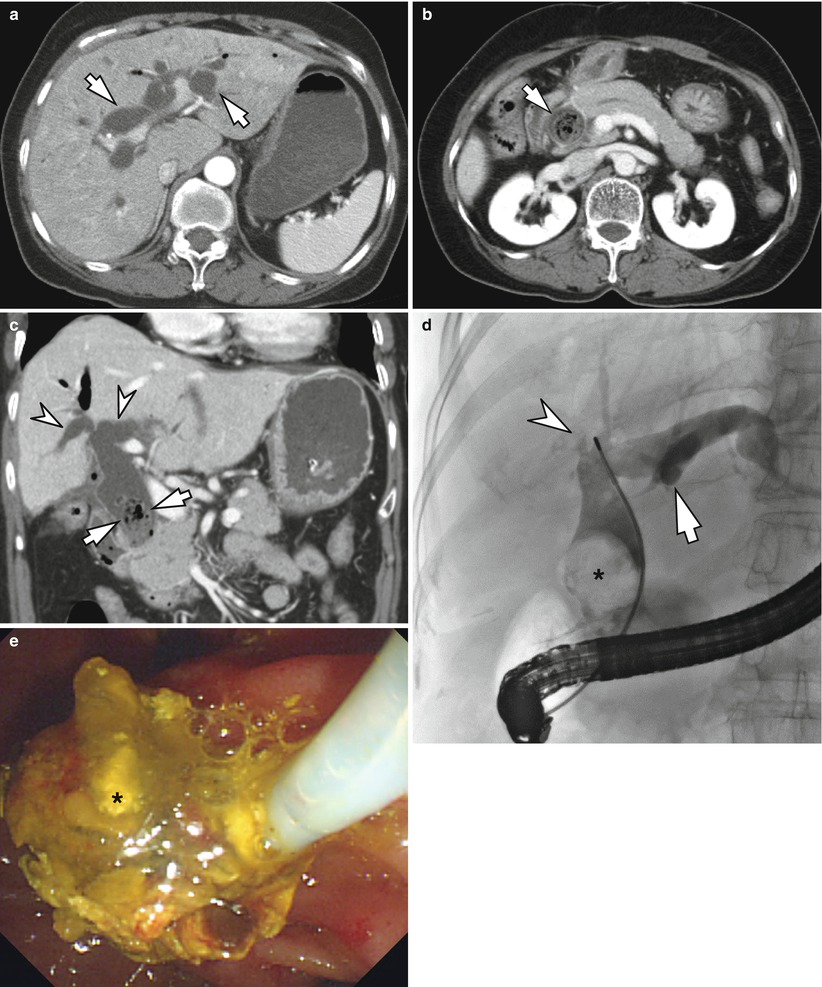
Fig. 12.7
Recurrent pyogenic cholangitis in a 66-year-old woman. (a) Contrast enhanced CT shows marked dilatation of both intrahepatic ducts (arrows). (b) More caudal scan reveals dilated common bile duct filled with air-bubble containing non-enhancing mass suggestive of muddy stone (arrow) with biliary obstruction. (c). Coronal image of CT shows muddy stone in the distal common bile duct (arrows) and dilated both intrahepatic ducts with decreased arborization, suggestive of pruned tree appearance in recurrent pyogenic cholangitis. (d). Cholangiography obtained from ERC shows ductal stone as filling defect (asterisk) with intrahepatic duct dilatation (arrow) and missing duct of right hepatic lobe due to stricture (arrowhead). (e) Endoscopy shows muddy stone removed from distal common bile duct (asterisk)
12.7.8 Recurrent Pyogenic Cholangitis
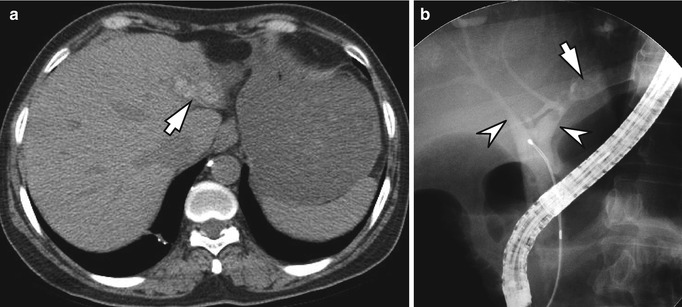
Fig. 12.8
Recurrent pyogenic cholangitis in a 57-year-old woman. (a) Noncontrast CT shows high-density stones impacted in the left lateral intrahepatic duct (arrow) with segmental hepatic parenchymal atrophy. (b) Cholangiography obtained from ERC shows dilated left lateral intrahepatic duct with filling defect due to stones (arrow). Central intrahepatic ducts show acute tapering (arrowheads), suggestive of pruned tree appearance
12.7.9 Recurrent Pyogenic Cholangitis
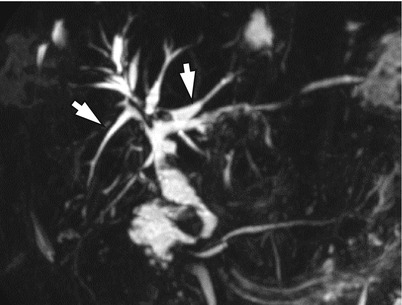
Fig. 12.9
Recurrent pyogenic cholangitis in a 68-year-old woman. (a) MRCP shows ductal rigidity and straightening, increased or right-angle branching pattern, and acute tapering of peripheral ducts (arrows), as well as focal strictures suggestive of recurrent pyogenic cholangitis
12.7.10 Cholangiocarcinoma Having Recurrent Pyogenic Cholangitis
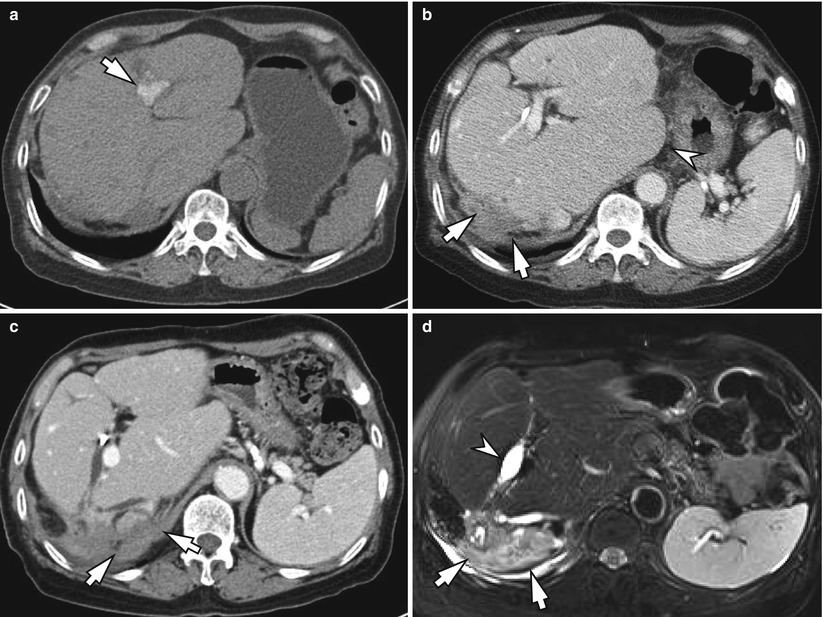
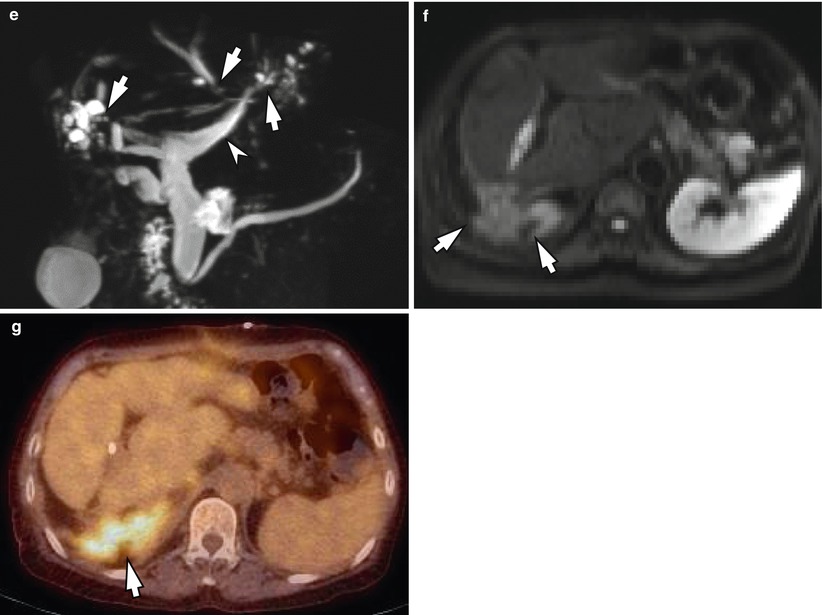
Fig. 12.10
Cholangiocarcinoma in a 71-year-old woman having recurrent pyogenic cholangitis. (a) Noncontrast CT shows stones in the intrahepatic duct (arrow). Right hepatic lobe is previously resected. (b) Portal phase CT shows infiltrative enhancing soft tissue along right hepatectomy resection margin with adjacent diaphragm invasion (arrows). Also note cirrhotic configuration of liver with hypertrophic caudate lobe (arrowhead). (c) More caudal scan reveals that the soft tissue infiltrates along inferior vena cava and suprarenal space (arrows). (d) T2-weighted MR shows infiltrative tumor as high signal intensity (arrows




Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
