KEY FACTS
Terminology
- •
Cholangiolithiasis, hepatolithiasis, biliary calculi, common bile duct (CBD) stones
Imaging
- •
Most stones are highly echogenic with posterior acoustic shadowing
- ○
Ultrasound is 1st-line imaging modality
- ○
Most common in periampullary region/distal CBD
- ○
- •
ERCP: Radiolucent, faceted, or angular filling defects within bile ducts
- ○
Gold standard is diagnostic and potentially therapeutic
- ○
- •
MRCP: Low-intensity filling defects within increased signal intensity bile ducts
- ○
Very sensitive for detection of bile duct stones
- ○
- •
NECT: Attenuation of stones varies from less than water density, through soft tissue, to dense calcification
- ○
Not very sensitive for detection of bile duct stones
- ○
Top Differential Diagnoses
- •
Cholangiocarcinoma, ampullary mass
- •
Ascending cholangitis, recurrent pyogenic cholangitis, or parasitic infection
Pathology
- •
Passage of gallstones into biliary ductal system (more common) vs. de novo stone formation within ducts
- •
Can cause obstruction with subsequent ductal dilation
Clinical Issues
- •
Presentation: Right upper quadrant pain, pruritus, jaundice; however, may be asymptomatic
- •
May present with acute complication: Cholangitis, pancreatitis
Scanning Tips
- •
Most stones will be located in distal CBD; extra effort is required to evaluate entire course of CBD to level of pancreatic head
- •
Acoustic shadow can be enhanced by using higher frequency transducers or turning off compound imaging
- •
Gain set too high can obscure posterior acoustic shadowing
 in the distal common bile duct (CBD)
in the distal common bile duct (CBD)  and gallbladder
and gallbladder  .
.
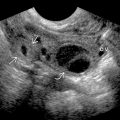
 with posterior shadowing
with posterior shadowing  that is compatible with a stone is present within the CBD
that is compatible with a stone is present within the CBD  on this longitudinal US. The CBD is located anterior to the hepatic artery
on this longitudinal US. The CBD is located anterior to the hepatic artery  and the portal vein
and the portal vein  . The hepatic artery crosses in between the portal vein and CBD.
. The hepatic artery crosses in between the portal vein and CBD.Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


