Chondral & Osteochondral Injury, Ankle
Julia Crim, MD
TERMINOLOGY
Definitions
Osteochondral lesion (OCL): Umbrella term for focal injury of articular cartilage and underlying bone
Preferred term, does not indicate chronicity or stage
Osteochondral injury: Term used for acute/subacute lesions
Osteochondritis dissecans (OCD): Chronic osteochondral lesion
Multiple staging systems used
Berndt and Harty staging system most widely accepted staging system
Stage 1: Subchondral bone bruise, injury to overlying cartilage
Stage 2: Crescentic fracture line, stable or partly detached
Stage 3: Detached osteochondral fragment, in situ
Stage 4: Detached osteochondral fragment, displaced from donor site
Stage 5 (later addition to classification, some classify this as 2A): Cystic degeneration of osteochondral fragment
Most important features to orthopedic surgeon are lesion size and stability
IMAGING FINDINGS
General Features
Location
Talus: Most commonly posteromedial or anterolateral
Tibial plafond: Variable location
Morphology
Lateral talar OCL: Usually shallow flake of avulsed bone and overlying cartilage
Medial talar OCL: Usually deep, rounded lesion due to compression
Radiographic Findings
Bowl-shaped fracture line exiting at joint surface
Rounded bony defect at articular surface
Cyst-like lucency beneath articular surface
Thin flake of bone from subchondral bone plate
MR Findings
MR arthrogram findings correlate reliably with Berndt and Harty surgical staging
Stage 1: Cartilage abnormality, bone marrow edema
Stage 2: Curved fracture line below cartilage (cartilage may normalize)
Stage 3: Arthrographic contrast extends below unstable fragment
Stage 4: Bone defect, may or may not see displaced fragment
Stage 5: Cyst-like area of low signal T1WI, high signal T2WI
Enhances with IV contrast due to fibrinous material filling “cyst”
Poor prognostic indicator for healing
CT Findings
CT arthrography: Similar to MR, but does not detect bone marrow edema
DIFFERENTIAL DIAGNOSIS
Subchondral Cyst due to Arthritis
Mimics cystic degeneration of OCL
Roughly spherical shape rather than bowl shape
Osteophytes, nonuniform cartilage thinning also present
Cartilage thins along lines of stress
Erosion due to Inflammatory Arthritis
Usually less sharply marginated
First erosions occur in bare area (margins) of joint
Uniform cartilage loss usually present
Avascular Necrosis
Subchondral bone marrow abnormality with serpentine margin
Cartilage normal until subchondral collapse occurs
PATHOLOGY
General Features
Etiology
Talus lesions due to inversion ankle injury
Tibial plafond injury: Impaction injury, due to inversion or axial load
May be single traumatic episode or chronic, repetitive trauma
Associated abnormalities
Talus OCL: Always associated with lateral collateral ligament injury
Tibial OCL: Lateral collateral injury or syndesmosis injury
CLINICAL ISSUES
Presentation
Most common signs/symptoms: Pain, clicking, locking
Natural History & Prognosis
May heal spontaneously
Complications: Collapse of articular surface, intraarticular loose bodies
Treatment
Drilling chondroplasty
Osteochondral allograft
SELECTED REFERENCES
1. De Smet AA et al: Value of MR imaging in staging osteochondral lesions of the talus (osteochondritis dissecans): results in 14 patients. AJR Am J Roentgenol. 154(3):555-8, 1990
2. Berndt AL et al: Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am. 41-A:988-1020, 1959
Image Gallery
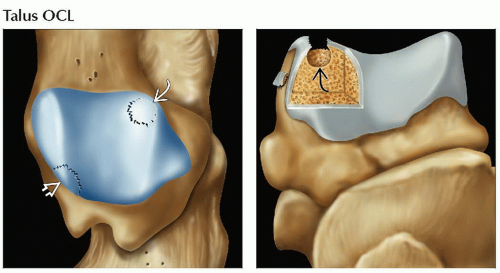 (Left) Graphic shows superior surface of talar dome with most common sites of OCL, both occurring from inversion injury. Posteromedial OCL  reflects impaction force on articular surface, and anterolateral OCL reflects impaction force on articular surface, and anterolateral OCL  reflects avulsive force. (Right) Graphic shows stage 4 OCL view from posterior view. A rounded osteochondral defect is seen reflects avulsive force. (Right) Graphic shows stage 4 OCL view from posterior view. A rounded osteochondral defect is seen  . Unlike subchondral cyst due to arthritis, the defect has a wide communication with the joint. . Unlike subchondral cyst due to arthritis, the defect has a wide communication with the joint. |
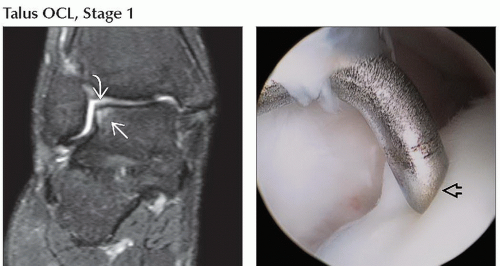 (Left) Coronal MR arthrogram T2WI FSE FS shows talar bone marrow edema
 and high signal intensity in overlying cartilage and high signal intensity in overlying cartilage  , stage 1 OCL. (Right) Frontal arthroscopic photograph in the same ankle shows a probe indenting , stage 1 OCL. (Right) Frontal arthroscopic photograph in the same ankle shows a probe indenting  softened cartilage. Cartilage appeared normal to visual inspection. softened cartilage. Cartilage appeared normal to visual inspection.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|