Renal failure includes a spectrum of diseases from acute and reversible to chronic and irreversible. Many long-standing renal diseases lead to the final state of decrease in renal size, parenchymal atrophy, glomerular sclerosis and fibrosis.
Definition and staging
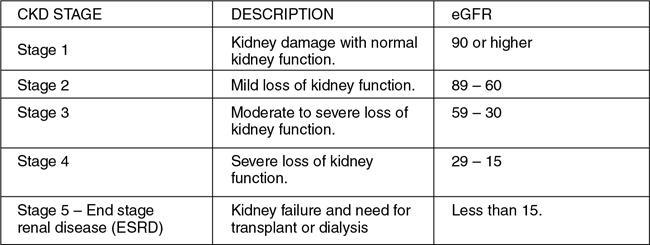
Chronic kidney disease is defined as deranged creatinine levels over few months to years and is based on the extent of kidney damage. It is estimated by a decrease in glomerular filtration rate (less than 60 mL/min per 1.7 m2) for more than three months (Fig. 10.12.3.3.1).
In a patient presenting with reduction in glomerular filtration rate (GFR), the treating physician must differentiate between an acute or chronic renal failure (CRF), and the clinical profile and laboratory parameters help make this differentiation. However, the laboratory abnormalities like anaemia, hypocalcaemia and hyperphosphataemia, which are characteristic of CRF and are also often present in patients with acute renal failure.
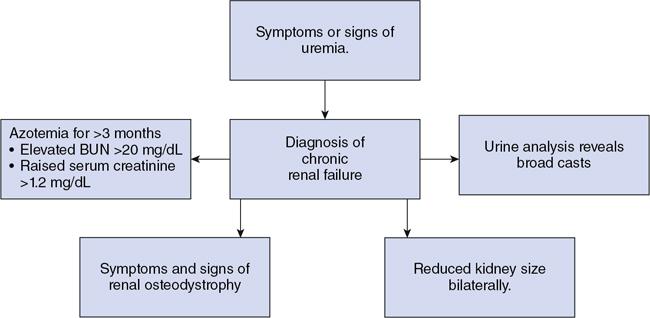
Hence a combination of the clinical signs and symptoms, laboratory parameters and radiological findings aid in the diagnosis of CRF (Fig. 10.12.3.3.2).
Fig. 10.12.3.3.2Flow chart describing the diagnostic finings of chronic renal failure.
Etiopathogenesis of chronic renal failure
Prerenal causes: Decreased renal perfusion accounts for 40%–80% of cases of acute renal failure and, if appropriately treated, is readily reversible. CRF may result following a prolonged long duration of the following causes:
4. Reduction in cardiac output from peripheral vasodilation: Sepsis, drugs.
5. Profound renal vasoconstriction: Severe heart failure, hepatorenal syndrome, agents such as nonsteroidal antiinflammatory drugs (NSAIDs).
Intrarenal causes: The common intrarenal causes of renal failure are diabetic nephropathy, hypertensive nephropathy and glomerulonephritis. Other causes are as listed below:
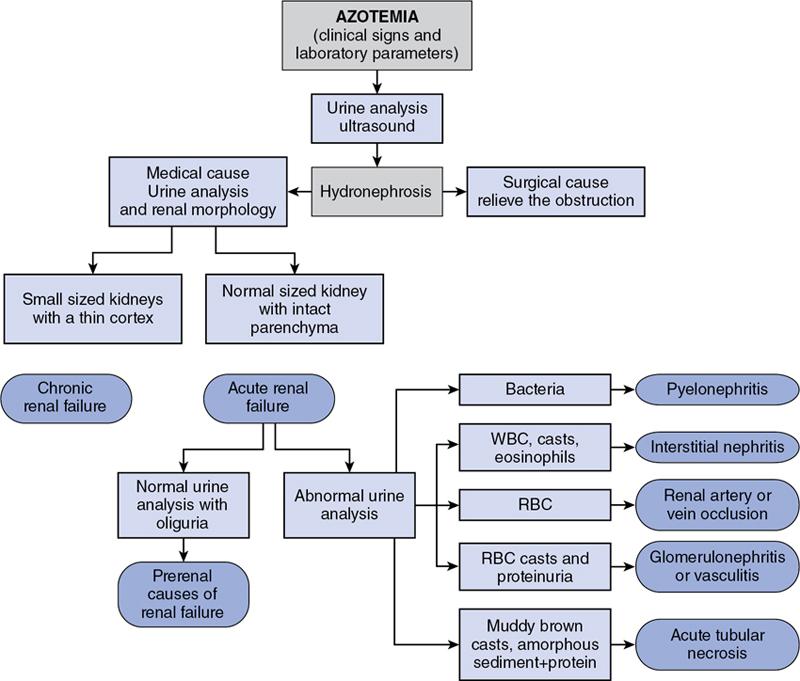
Approach to renal parenchymal diseases: The following flow chart demonstrates the algorithmic approach to a case of renal parenchymal disease (Fig. 10.12.3.3.3).
Fig. 10.12.3.3.3Flow chart depicting an approach to renal parenchymal diseases.
Role of imaging in chronic renal failure
Imaging helps the clinician:
1. To differentiate between a surgical and medical condition (to primarily exclude obstruction).
2. To distinguish between acute and chronic renal injury.
3. To gauge the extent of renal damage.
Renal parenchymal diseases presents with a varied clinical picture and imaging findings which may be nonspecific. Renal biopsy is often required for a specific diagnosis.
A multimodality approach often helps in reaching a diagnosis for a particular case. Hence, it is important to know the benefits and the limitations of each modality.
1. Radiography: Plain radiographs and intravenous urography
Plain X-ray KUB may reveal the following findings:
a. Calcifications: To identify parenchymal calcifications, calculi and renal vascular calcifications.
b. Renal outline: This determines the size of the kidney. Normal renal size is approximately equal to 3–4 lumbar vertebral body height.
c. Renal osteodystrophy: Long-standing cases of renal failure may show bony changes which are best seen in the bony pelvis and spine.
Intravenous Urography (IVU):
IVU is generally not used in renal failure due to the possibility of worsening of renal function by contrast agents, particularly with the advent of other imaging modalities like ultrasound.
In both acute and chronic renal failure, there is slow and diminished initial opacification of the renal cortex and the washout occurs at a slower rate as compared to a normal kidney. Following administration of the same contrast dose in normal patients and end-stage renal disease (ESRD), the densest opacification of the cortical or medullary tissue is never the same which is probably due to a diminished GFR and concentrating capacity of the remaining tubules.
On IVU, interesting abnormal nephrographic patterns are seen first described by Fry and Cattell, which are:
3. Immediate dense persistent nephrogram – Acute tubular necrosis and severe inflammatory renal disease.
4. Striated nephrogram – It is a variant of obstructive nephrogram which may also be encountered in other conditions like pyelonephritis, PAN, trauma and medullary cystic kidney disease.
Only gold members can continue reading. Log In or Register to continue