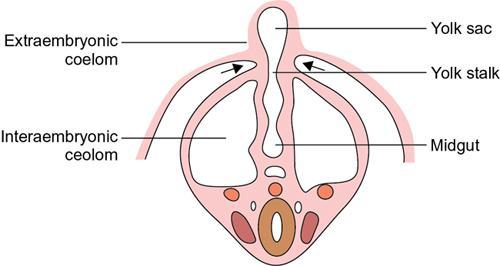
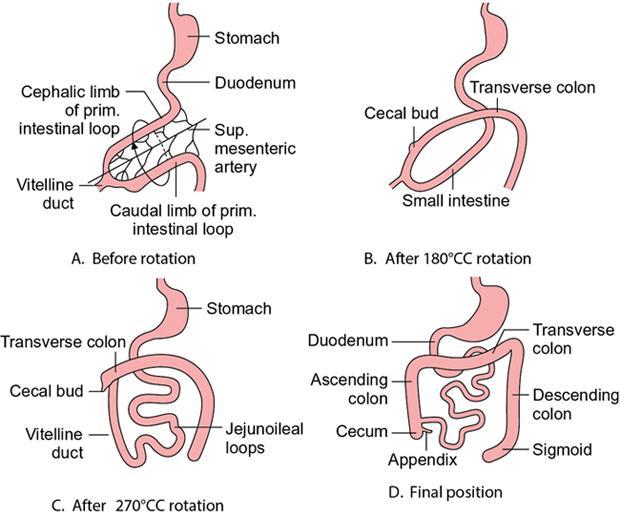
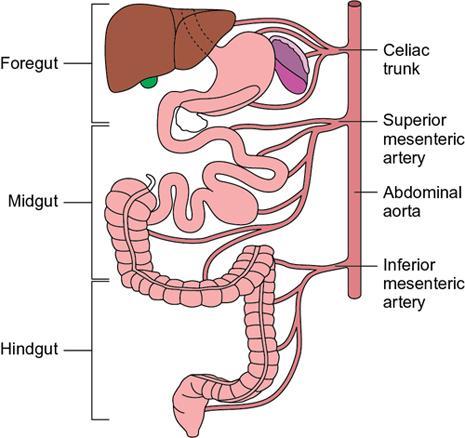
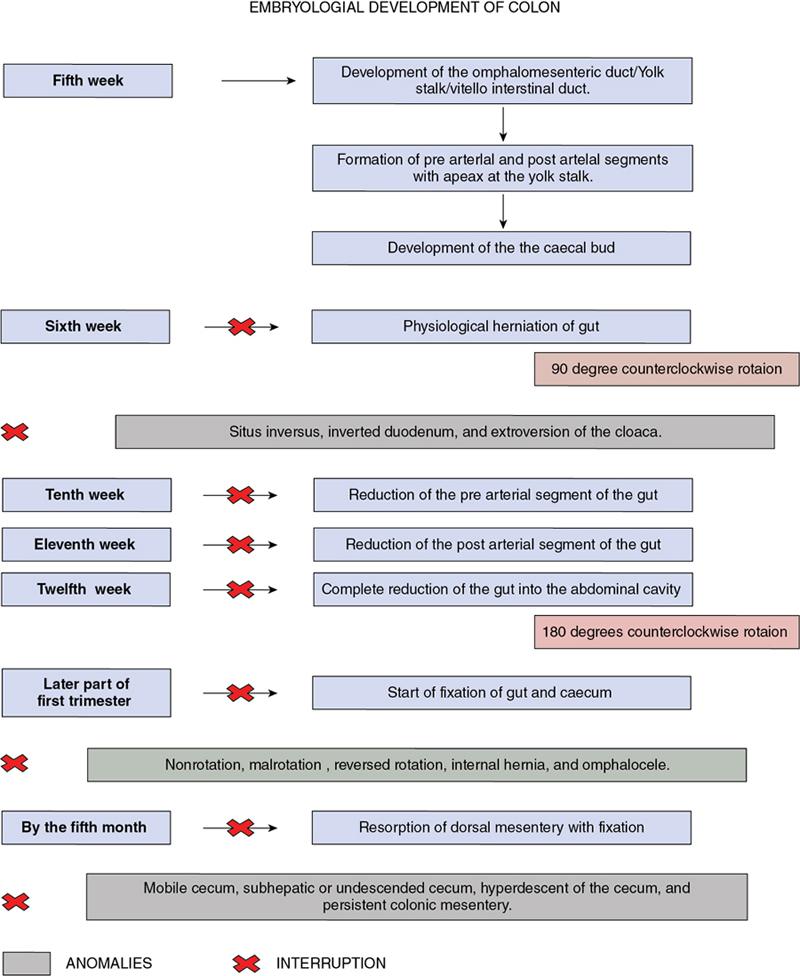
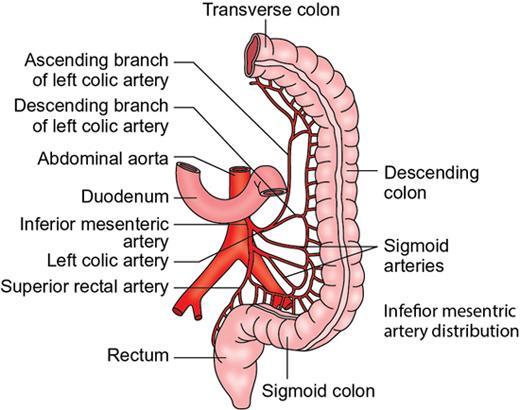
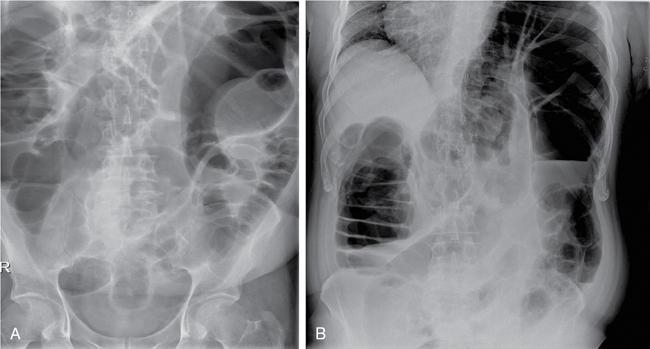
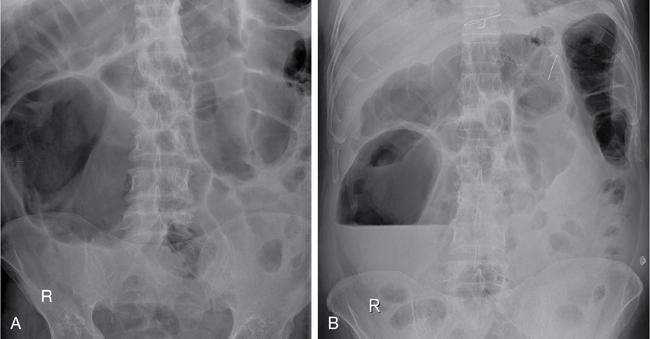
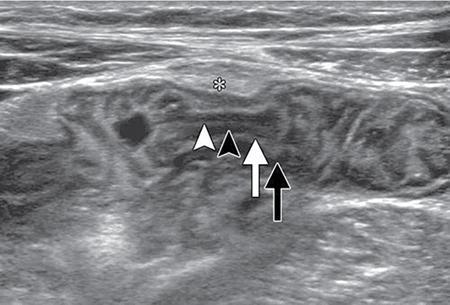
Kulbir Ahlawat, Ravi Chaudhary, Arvind Pandey, Anuj Bahl, Navni Garg, Sonam Shah, Sonali Sharma EMBRIOLOGY AND ANATOMY OF COLON Sonali Sharma A deep understanding of the development and the embryology of the colon is essential to understand the variety of the developmental anomalies related to the aberrations in the normal embryological processes (Table 8.4.1.1). Broadly the development of the colon can be summarized in three stages: The rate of growth of the embryo exceeds the growth rate of the yolk sac during the third and the fourth weeks of development. During the fifth week there is development of the omphalomesenteric duct or the Vitello intestinal duct or the yolk stalk which serves as a connection between the extraembryonic and the intraembryonic coelom (Fig. 8.4.1.1). The midgut at this point is divided into two equal length segments and the loop has its axis at the superior mesenteric artery (SMA). The apex is marked by the yolk stalk or the omphalomesenteric duct. There is a periarterial segment and the postarterial segment of the loop, the former starting at the foregut–midgut junction and ending at the apex. The postarterial segment lies between the apex and the midgut–hindgut junction. Eleventh week marks the beginning of the return of the postarterial segment of the gut, which continues to rotate in front and then to the right of the SMA. By the twelfth week the colon completes a 270-degree anticlockwise rotation with prior 90 degrees during herniation, and a further 180-degree counterclockwise rotation during the reduction of the postarterial segment. The prearterial segment gives rise to: Postpapillary duodenum, jejunum, ileum (major part) The postarterial segment gives rise to: Terminal ileum, caecum, appendix, ascending colon, transverse colon (major part) There is a switch over to the hind gut at the junction of the proximal two-thirds and the distal one-third of the transverse colon where there is also a switch over in the arteries supplying the segments, with SMA (middle colic) supplying the proximal segment and the inferior mesenteric artery (IMA, left colic) supplying the distal segment. The fifth week also marks the development of a small swelling in the proximal postarterial segment which represents the caecal bud. There is the herniation of the midgut at the sixth week of development called the physiological herniation of the gut. At this time there is growth of the liver, and the right lobe pushes the prearterial segment downwards and to the right. The series of events represent a 90-degree counterclockwise rotation when viewed enface (Fig. 8.4.1.2). The anomalies of this stage (stage of physiological herniation) are rare and include situs inversus, inverted duodenum and extroversion of the cloaca. With growth of the peritoneal cavity and no further significant growth of the liver, there develops a free space within the peritoneal cavity for the reduction of the midgut hernia at about the tenth week of development. Eleventh week marks the beginning of the return of the postarterial segment of the gut, which continues to rotate in front and then to the right of the SMA. By the twelfth week the colon completes a 270-degree anticlockwise rotation with prior 90 degrees during herniation, and a further 180-degree counterclockwise rotation during the reduction of the postarterial segment (Fig. 8.4.1.2). There occurs the fixation of the gut in this final sequence of events which start towards the later part of the first trimester. Anomalies of the reduction phase of the physiological hernia are relatively more common than the ones that originate from the stage of physiological hernia and include nonrotation, malrotation, reversed rotation, internal hernia and omphalocele (Fig. 8.4.1.3). There is a discrepancy in the growth rates of the base of the caecum and the apex of the caecum which leads to the formation of an appendage called the appendix. Further till the fifth month of gestation there is a progressive gradual resorption of the dorsal mesentery. Gradually, fusion of parts of the primitive mesentery occurs, with fixation of the duodenum, and the ascending and descending parts of the colon to the posterior abdominal wall in their final position. Anomalies of this stage of fixation are common and include mobile caecum, subhepatic or undescended caecum, hyperdescent of the caecum and persistent colonic mesentery (Fig. 8.4.1.3). The mesentery of the transverse colon (mesocolon) persists with its partial fusion with the greater omentum leading to the formation of the gastrocolic ligament. The distal end of the transverse mesocolon condenses to form the phrenicocolic ligament, which suspends the transverse colon near the splenic flexure fixing it to the diaphragm in the left upper abdomen. It also prevents the spread of pathologies from the left paracolic gutters to the left upper abdomen. The sigmoid colon continues to maintain it dorsal mesentery or sigmoid mesocolon at its posterior aspect. The length of the mesentery is short relative to the variable length (sometimes very long) of the colon to which it is attached. This discrepancy leads to the sigmoid volvulus. Colon is formed from the midgut and the hind gut with the junction of the proximal two-thirds and distal one-third of the transverse colon being the point of demarcation between the two. The midgut development continues beyond the opening of the papilla, to form the duodenum beyond the papilla, ascending colon and the proximal two-thirds of the transverse colon. This segment is supplied by the Superior Mesenteric Artery with corresponding venous and lymphatic drainage (Fig. 8.4.1.4). The distal third of the transverse colon, descending colon, sigmoid colon, rectum and the anal canal above the dentate line all are derived from the hind gut and supplied by the Inferior Mesenteric Artery with corresponding venous drainage and lymphatics (Fig. 8.4.1.3). Enteric nervous system (ENS) functions independent of the CNS and is thus referred to as the ‘Second Brain’ and it regulates many aspects of gastrointestinal physiology including peristalsis, sphincter tone, glandular secretions, smooth muscle activity and microcirculation. The neuroenteric ganglion cells migrate from the neural crest to the upper end of the alimentary tract and then follow vagal fibres caudad during the first trimester. The ENS is composed of two types of ganglionated plexuses: the Auerbach (myenteric) plexus, which is located in the outer muscular layer and regulates gastrointestinal tract motility and function of extraluminal organs, and the Meissner (submucosal) plexus, which regulates enteral secretory activity. In contrast to the neural crest-derived cells of the enteric plexuses, interstitial cells of Cajal (ICCS), which serve as the ‘pacemakers of the intestine’, arise from intestinal mesenchyme. Sympathetic innervation: L2–L5 roots, inferior and superior mesenteric plexus and coeliac ganglia. Parasympathetic innervation: The Vagus nerve and sacral spinal cord (S2–S4 spinal nerves). Great details of the various disorders are beyond the scope of this book. A short review is written (Table 8.4.1.2). Duodenal atresia (11%) – most common Meckel’s diverticulum (11%) – second commonest Omphalocele (9%) Other stenosis or atresia (5%) Hirschsprung’s disease (2%). Cardiac and orthopaedic anomalies Biliary atresia Pancreatic anomalies Microcolon Esophageal webs Tracheoesophageal fistula It is commonly known as malrotation and occurs due to an arrest of the first 90 degrees rotation of the midgut which causes the prearterial segment to lie to the right of the hernial sac and SMA and the postarterial segment to the left. The dorsal mesentery lies in the midline and is shared by both the pre and the postarterial segments. This makes the bowel loops imbalanced and mobile and prone to volvulus. The twisting of the midgut loop can occur mostly at the level of the duodenojejunal junction and less commonly at the level of the midtransverse colon. There is a disruption of the normal SMA to SMV relationship, with the SMV seen to the left of the SMA in this pathology. In this there is a reversal of the sequence of return of the midgut with postarterial segment returning first and lying posterior to the SMA with the duodenum and the small bowel lying anterior to the colon. Abnormal mesenteric bands may form leading to obstruction. Failure of the midgut to retract into the abdominal cavity with retention in the hernial sac. The colon may fail to complete its final 180-degree rotation and lie in the right upper quadrant. Incomplete resorption of the mesentery may lead to abnormally mobile colon segments due to centrally placed dorsal mesentery. It is interesting to know that the rotation anomaly of the prearterial segment may be an isolated entity but, the rotation anomaly of the postarterial segment is invariably associated with the anomaly of the prearterial segment. Caecum is an intraperitoneal organ either almost completely invested with peritoneum or at least invested by it in its lower half. It is fixed by a small mesocaecum. In 5% individuals the caecum rests directly on the iliacus muscle and the psoas major muscle due to lack of the peritoneum. Also, an abnormally mobile caecum and ascending colon may be seen in about 10%–22% individuals usually due to a long mesentery. Thus varied locations of the caecum may be seen. This is a fixation anomaly and may lead to a volvulus. This exclusively affects the postarterial segment with normal mobility and position of the prearterial segment. The caecum may lie in the left upper quadrant. Errors in the resorption of the dorsal mesentry, may lead to development of abnormal fossae through which the loops of the bowel may herniate (Fig. 8.4.1.5). Few common ones are detailed below: It formed the incomplete fusion of the mesentry of the descending colon. The bowel loops may herniate under the colon and in front of the IMA. This leads to the left paraduodenal internal hernia. A defect in the small bowel mesentery leads to herniation of the loops in the left upper quadrant, beneath the SMA to the right. This is called the right preduodenal hernia and is less common the left preduodenal hernia. Work on the anatomy of the colon dates back to the 16th century with the pioneering work of Andreas Vesalius. The versatile and ever evolving radiological procedures have further added to this knowledge over the past few decades, improving our understanding of this organ. There are no two opinions on the vital functions of absorption of nutrients, water and electrolytes and transmission and storage of residue performed by this organ. The colon is a long tubular conduit with variable length in different individuals, measuring approximately 120–200 cm (Table 8.4.1.3). Large bowel is differentiated from the small intestine structurally due to its unique longitudinal muscular bands called taenia and characteristic macroscopic saccular appearance and haustral pattern and Appendices Epiploic (Fig. 8.4.1.6). The saccular appearance is attributed to the shorter length of the longitudinal muscle fibre bands or taenia, which are about one-sixth shorter in length than the length of the colon per se. Also the haustral pattern or segmented appearance seen in the colon is characteristic, wherein the haustra are separated by the semilunar cresentric incomplete folds known as plicae semilunaris which may be better visualized when appropriate colonic distension is obtained by barium or air insufflation. The colon also has circumferential folds extending around the luminal surface called the plicae circularis, also seen in the small intestine where they represent folds of the mucus membrane. Thus, the plicae circularis are not exclusive to the colon. The longitudinal muscle bands called the taenia coli run along the serosal surface of the colon, and arrange into three muscle bands namely taenia liberis, taenia omentalis and taenia mesocolica, that are located 120 degrees from each other, and run from the caecum to proximal rectum. Taenia omentalis runs posterolaterally and is attached to greater omentum, taenia mesocolica runs posteromedially and is attached to mesocolic taenia and taenia liberis is boundless and runs anteriorly. At the rectosigmoid junction, taenia expands to cover the rectum. At the level of the sacral promontry there is gradual transition between the colon and the rectum, with confluent muscle fibres giving the rectum a Taenia Free appearance. It is worthwhile here to mention briefly the Appendice epiploicae which are exclusive to the colon and not seen in the small intestine as well as rectum and beyond. These are fatty appendages which perform the fat storage reserve function and are located along the serosal surface of the colon. Inflammation of these is now a disclosed entity frequently encountered in the radiological practice. The colon is divided into the caecum including the vermiform appendix, ascending colon, transverse colon, descending colon and the sigmoid colon (Fig. 8.4.1.7). The ascending colon and the descending colon are retroperitoneal, while the caecum, transverse colon and the sigmoid colon are intraperitoneal. The caecum is the widest part of the colon measuring 7.5 cm in diameter while the sigmoid colon is the narrowest part measuring 2.5 cm. It is due to this reason that the caecal masses acquire a very large size before causing obstructive symptoms and present later in the course of disease while the sigmoid colon masses present earlier in the course of the disease with obstructive symptoms. At the posteromedial aspect of the caecal wall two elliptical folds form the orifice for the ileocaecal valve which is formed by the circular muscle layers of terminal ileum and has a typical nipple like appearance. Some authors have suggested that an intact ileocaecal valve is advantageous in patients of short bowel syndrome by increasing the absorption of the nutrients. The ileocaecal valve appears mostly incompetent on the Barium Enema. However, a competent valve is known to prevent colonic decompression in patients of high-grade colonic obstruction. The Vermiform Appendix is a blind-ended tubular appendage arising from the caecal wall at its base posteromedially. It lies mostly intraperitoneally (95%). It is more commonly directed medially towards the ileum, retro caecally or alternatively in the lesser pelvis. Apart from these commonest locations, the appendix may be subcaecal (31%), transverse retrocaecal (2%), paracaecal, preileal (1%) and ascending paracaecal retroileal/postileal (0.5%). Appendix lacks taeniae, haustra, plicae semilunaris and appendices epiploicae and is located at the site of confluence of the three taenia. The appendix can be variable in length ranging 2–20 cm. It is interesting to note that clinically an intraperitoneal appendix is more symptomatic due to inflammation of the parietal peritoneum as opposed to a retrocaecal appendix. The ascending colon is short measures 10–20 cm and lies within the anterior pararenal space. The ascending colon is a (secondarily) retroperitoneal structure covered only on its ventral and lateral surfaces by the posterior peritoneum, with the mesocolon fused with the retroperitoneum. The ascending mesocolon is not a real mesentery because it is not formed by two peritoneal layers suspending the colon. The ascending mesocolon follows the course of the ileocolic vessels and marginal vessels along the mesocolic side of the colon. As the ascending colon reaches the liver, it turns 90 degrees at the curve called the hepatic flexure to continue across the upper abdomen to the left side to form the transverse colon up to the spleen where it curves to form the splenic flexure. The colon is completely wrapped by the peritoneum at the site of junction of the hepatic flexure and the transverse colon. Transverse colon is the longest part of the colon measuring about 40–50 cm in length. Transverse colon is the most mobile part of the colon due to its well-developed mesentery and may even reach up to the pelvis. It is attached to the diaphragm by the phrenicocolic ligament. Transverse colon is an intraperitoneal segment of the colon. The greater omentum is fused to the taenia mesolica at the inferior surface of the transverse colon. Beyond the splenic flexure the colon turns inferiorly to continue as the descending colon which is (secondarily) retroperitoneal, immobile and measures approximately 25–45 cm. The descending colon reaches the left iliac fossa where it continues as the S-shaped sigmoid colon which has the caudal end at the level of S3 vertebra. The sigmoid colon is attached to the pelvis by the sigmoid mesocolon and is completely invested by the peritoneum. The sigmoid mesocolon has long length and is tortuous and these features make the sigmoid colon prone to volvulus. The sweep of the sigmoid colon into the pelvis can range from gentle to an omega loop to a redundant coiled appearance. These variations and looping tendency in the sigmoid colon make it a difficult part to evaluate at colonoscopy. It is an interesting fact the rectosigmoid region acts as a functional sphincter due to sharp angulation in this region along with narrow luminal diameter thereby increasing the transit of residue across this region and thereby increasing the intrasigmoid pressure making it prone to diverticulosis. The colon is supplied by the SMA and the IMA which are branches of the abdominal aorta. The SMA gives rise to 12–20 jejunal and ileal branches and then continuing as the ileocolic trunk shifting further to the right towards the caecum. The ileocolic artery is a relatively constant artery with not many variations in the course. The SMA gives rise to the right colic artery (RCA) and the middle colic artery (MCA) which may show variations (Fig. 8.4.1.8). The IMA bifurcates into an ascending branch and a descending branch. The descending branch runs caudally and supplies the descending colon (Fig. 8.4.1.9). In the pelvis it gives 2–6 sigmoidal arteries and becomes the superior haemorrhoidal artery also called the superior rectal artery. The anterior branch ascends and contributes to the formation of the Arc of Roilan. It is interesting to know that while most of the blood supply off the colon is segmental, the sigmoidal arteries form an arcade that is similar to the small bowel vasculature and have multiple anastomosis. It corresponds to the arteries. The marginal artery of Drummond is called the central anastomotic artery, runs along the entire medial aspect of the colon and provides the collateral circulation between the SMA and the IMA. A watershed zone called the Griffiths Critical Zone is seen at the junction of the proximal two-thirds and the distal one-third of the transverse colon which is the site between the blood supply by the SMA and the IMA branches is also the site where the midgut joins the hind gut. Another area of diminished blood supply is called the Sudeck’s point which is located near the rectosigmoid Junction. It is a point of anastomosis between the IMA and the internal iliac artery. There is another thick meandering artery called the Arc of Riolan that plays a critical role in providing collateral circulation between middle colic artery and the ascending branch of the left colic artery when either the SMA or IMA is occluded. The vasa recta supply the colonic lumen. The colon has a rich lymphatic supply, typically divided into: The sympathetic supply of the right colon originates from lower thoracic segments. They synapse with preaortic, coeliac and superior mesenteric ganglia. Parasympathetic supply is from the right Vagus nerve branch and the coeliac plexus. The sympathetic nerves supplying the left colon and rectum arise from L1 to L3. The large intestine measures about 60 cm in length. The muscularis is very poorly developed. The ascending and descending colon are relatively shorter than the transverse colon. The normal haustra and appendices epiploic are not present, giving the paediatric colon a very smooth outline. The haustra appear over the first 6 months of birth. IMAGING TECHNIQUES FOR COLON Navni Garg, Ravi Chaudhary Plain abdominal radiograph is usually the first imaging investigation requested in patients suspected of bowel obstruction and/or perforation. They aid in differentiating small bowel obstruction from large bowel obstruction (LBO). Specific signs on a plain radiograph prompt the radiologist towards considering particular aetiology. Various indications of abdominal radiograph are enlisted in Table 8.4.2.1. The abdominal radiography usually involves a supine radiograph (anteroposterior projection) and should include the diaphragm superiorly and ischial tuberosities inferiorly. An additional horizontal beam (upright, decubitus, or cross-table lateral) projection may be done where obstruction/perforation is suspected to detect small amounts of pneumoperitoneum and evaluate air–fluid levels. Some institutions prefer to perform an upright chest radiograph to detect small amount of intraperitoneal free gas. Horizontal beam radiographs should always be performed after placing the patient in upright or decubitus position for at least 5 minutes before exposing the radiograph. The size of the film or image receptor varies with the size of the patient. In adults, a 14 × 17 inch film is usually appropriate. Radiographs are usually taken at end expiration, wherever possible using low kVp (60–75 kVp). However, technical parameters are usually varied according to patient size. Few of the important indications are discussed here: Adynamic ileus is generalized dilatation of small and large bowel loops and is different from pseudo-obstruction as there are no chances of perforation in ileus. Frank distension of rectum implies ileus. Air–fluid levels not seen in pseudo-obstruction or ileus and favour obstruction. It is important to rationalize the use of radiographs and perform alternative radiation free modality like ultrasound wherever possible. USG is often the first modality used for imaging patients with abdominal pain. It is an inexpensive and widely available modality for abdominal imaging. However, limitations such as operator experience, patient’s body habitus, bowel gas–related artefacts and patient cooperation preclude the wide use of this noninvasive modality for imaging of colonic pathologies. Destruction of gut signature is harbinger of some malignant process, more so if length of bowel involved is short. However, aggressive inflammatory processes may also cause focal disruption of gut. Normally diseased bowel segment is better appreciated on USG due to reduced motility and thickened walls are larger and easier to see. Further, colour Doppler can be used to assess mural vascularity however due to low blood flow in the mural vessels and artefacts due to peristalsis, it may not always be possible to document hyper- or hypovascularity. Mural hypervascularity is usually seen in inflammatory or infectious diseases whereas hypovascularity in thickened bowel is suspicious of ischaemia. The guidelines of the European Federation of Societies for Ultrasound in Medicine and Biology have specified indications for the use of CEUS in IBD cases: Limitation of CEUS is bowel motility which leads to suboptimal imaging quality and only limited segment is evaluated at a time. Though CT is more reliable imaging modality in patients with diverticulitis, USG is helpful in early, uncomplicated diverticulitis especially in lean patients. Even with the advent of advanced imaging techniques, contrast enema continues to provide relevant information to clinicians and surgeons. The aim is to obtain good-quality images with various projections and least radiation exposure. Various indications and contraindications of contrast enema are enlisted in Table 8.4.2.2. Patient is advised to consume low-residue diet for previous 2 days and laxative a day before the examination. In our centre, two scout views are taken before contrast administration: AP abdomen and left lateral pelvis to check for adequate bowel preparation and rule out any obstruction/perforation. This is followed by introduction of a rectal tube lubricated with lidocaine jelly through the anal opening, taped to the sides and connected to an enema bag hanged on an IV pole. Either barium or water-soluble contrast can be used. Water-soluble contrast is used in patients with suspected colonic obstruction or volvulus, early postsurgical patients where perforation/leak is suspected or where Blind-ending colonic segments (e.g. rectal remnant following the Hartmann procedure or J-pouch) are present. It is also recommended in patients with distal intestinal obstruction syndrome/meconium ileus equivalent in patients with cystic fibrosis to demonstrate the level of the obstruction and possibly be therapeutic. Repeat enemas with water-soluble contrast agents over several days may be required to mobilize the tenacious stool plugs. Water-soluble contrast contains 300–370 mg of iodine/mL, equivalent to 60%–76% density. It may be diluted with water to 20%–30%, depending on the indication. For visualization of water-soluble contrast, kilovoltage of 70–80 kVp should be used during image acquisition. Contrast enema can be performed as single contrast or double contrast study. Single contrast study allows real-time imaging of colonic leaks and fistulas in inflammatory bowel diseases (IBDs) and postoperative patients whereas double contrast study provides better mucosal information in patients with failed colonoscopy for screening of colorectal malignancy. Single contrast study involves use of 20% w/v of barium. A kilovoltage of 100 kVp or greater should be used (depending on patient size) during image acquisition. Barium is allowed to flow and patient is turned to facilitate the passage of barium till it reaches the caecum and the ileocaecal valve (and possibly the appendix). Spot radiographs are taken intermittently to demonstrate each loop of colon with adequate barium coating and distension (Figs. 8.4.2.10–8.4.2.13). Manual or mechanical compression should be applied as appropriate to all accessible segments of the colon during fluoroscopy. Images should include (ACR Guidelines):
8.4: Colon
Embryology of colon
Development of the appendix
Colonic blood supply basics
Nervous system of the colon
Nerve supply
Common anomalies related to development
The anomalies of rotation and fixation may be associated with multiple other anomalies listed below.
COMMON ANOMALIES
LESS COMMON ANOMALIES
PROXIMAL COLON DUPLICATION
These include three anomalies:
Nonrotation
Reversed rotation
Omphalocele
Incomplete rotation and malfixation anomalies
Incomplete attachment of the caecum and mesentery
Hyperrotation
Internal herniations
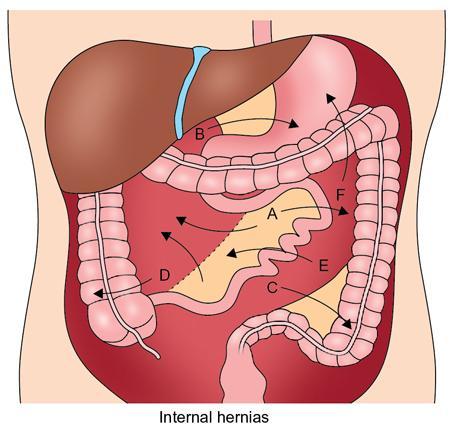
Fossa of landzert
Fossa of waldeyer or mesentericoparietal fossa
Defect in the sigmoid mesocolon and transverse colon mesentery
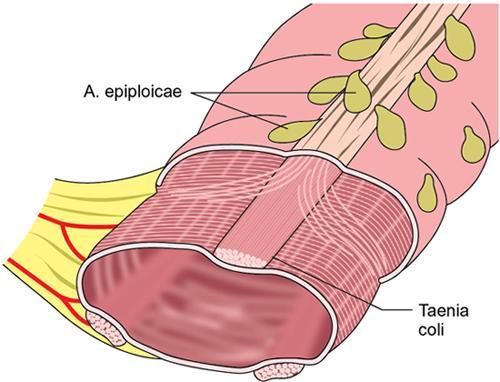
Anatomy of colon – a brief insight
How to identify the large bowel?
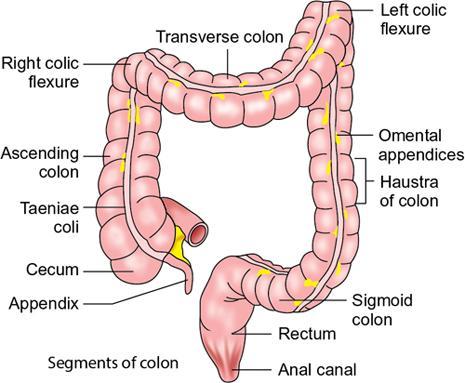
Segments of the colon
Why is sigmoid colon the commonest site of diverticulosis in the large bowel?
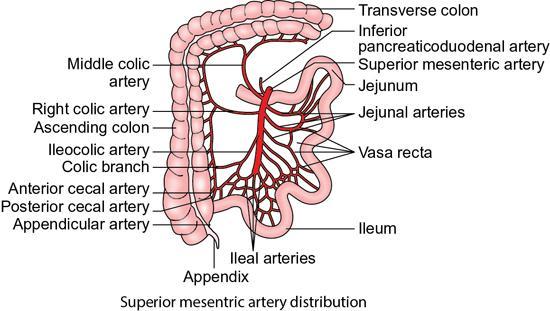
Blood supply of the colon
Arterial supply
Venous supply
Collateral circulation in the colon – a protective mechanism
Lymphatics
Nerve supply
Paediatric colon anatomy
Plain abdominal radiograph
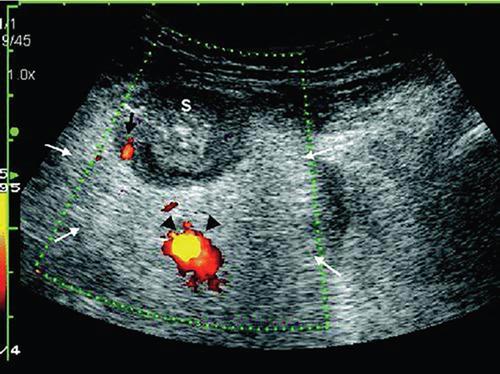
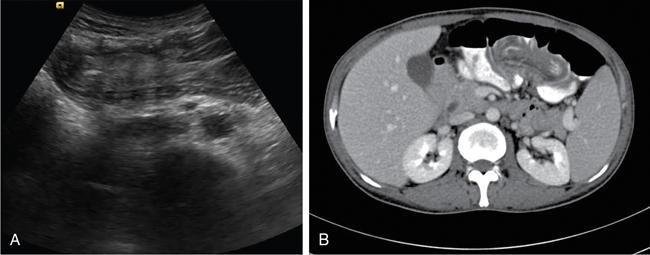
Ultrasonography (USG)




Contrast enema
Technique
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


