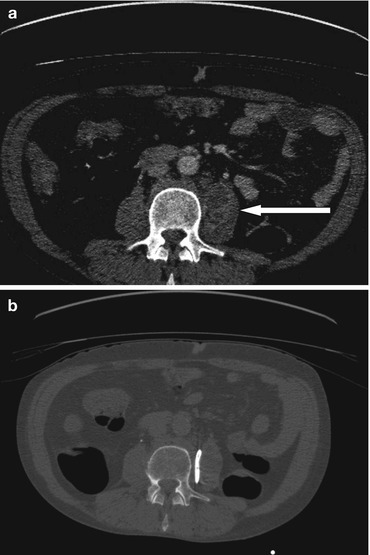
Fig. 3.1
(a) Axial image from a CT in an 85 year old female with severe upper abdominal pain and peritonitis in whom chest and plain abdominal radiographs were normal. This shows a shallow collection of air anterior to the liver surface in the right upper quadrant, outside the confines of the colonic lumen. The average attenuation value was −965 Hounsfield units (HU), comparable to the attenuation value of air outside the patient at the top right periphery of the image which averaged −992 HU. (b) Axial CT image through the upper abdomen in a 66 year old female patient with a history of metastatic ovarian carcinoma and peritoneal carcinomatosis. There is extensive free fluid surrounding the liver and spleen as well as a large volume of fluid in the left pleural space. The average attenuation value of the fluid ranged from 7 to 11 HU, consistent with malignant ascites and malignant pleural effusion
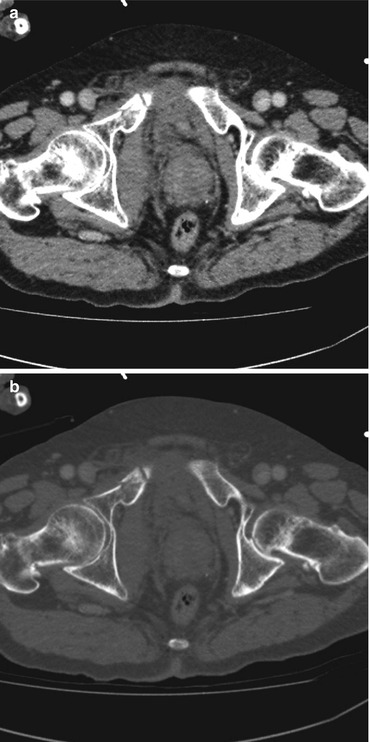
Fig. 3.2
Axial CT images at the level of the pubic rami in a 76 year old male patient who sustained blunt pelvic trauma viewed on (a) a soft tissue window and (b) a bone window, reveal right sided pubic rami fractures. The fractures are much better delineated on appropriate windowing (b), optimised for detection of osseous fractures and osseous destructive lesions
Indications
CT is a valuable technique in all body systems:
Chest – it may be indicated in problem solving abnormalities identified on plain film particularly where there is a discrepancy between the clinical and imaging findings, for example in the post-operative patient in whom chest x-ray frequently demonstrates bibasal infective consolidation and effusion but who are at high risk for concurrent venous thromboembolism (Fig. 3.3a, b), in the immunocompromised patient subgroup including those with chronic illness in whom there is an increased risk of atypical respiratory tract infection such as TB (Fig. 3.4a–c), fungal infection and cavitating infection. CT can be a critical adjunct to the chest x-ray in these select subgroups of patients, without which important underlying or co-existing pathology would have a delayed clinical diagnosis.
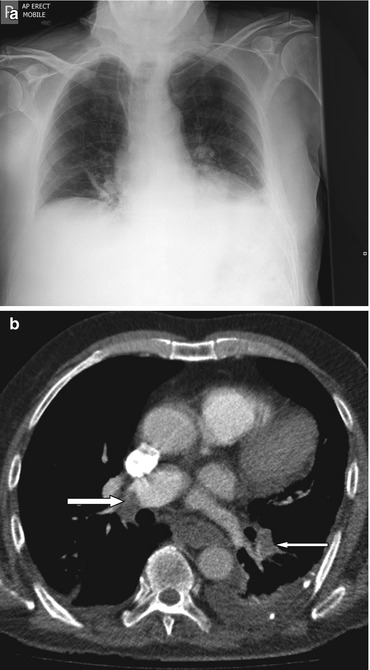
Fig. 3.3
(a) Chest x-ray in a 73 year old male patient re-admitted 2 weeks following radical prostatectomy with shortness of breath, low-grade pyrexia and an elevated white cell count, thought clinically to represent a post-operative pneumonia. X-ray showed patchy atelectasis in the right middle lobe with left lower lobe consolidation. He failed to improve clinically despite 48 h of intravenous antibiotics and a CT pulmonary angiogram was subsequently performed. (b) CT pulmonary angiogram in the same patient demonstrates filling defects within the right main and left lower lobe pulmonary arterial branches (arrows) consistent with acute pulmonary embolus in addition to bibasal consolidation and effusion
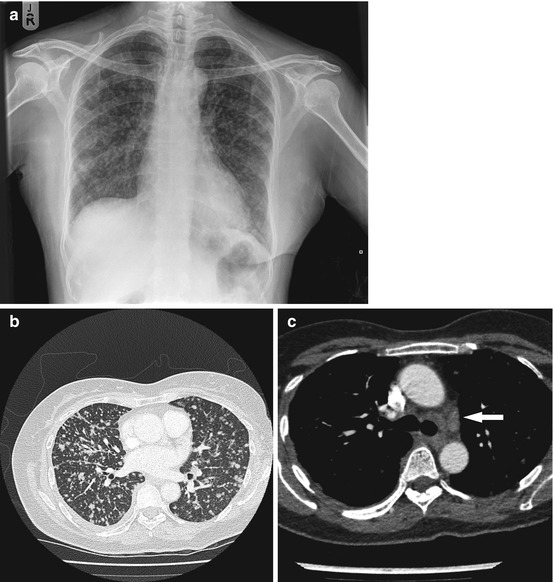
Fig. 3.4
(a) Chest x-ray in a 53 year old female patient who presented with a 1 month history of cough and weight loss on a background of HIV positivity shows multiple bilateral nodules measuring up to 5 mm in diameter. The differential was between miliary TB and miliary metastases. (b, c) Further evaluation with CT of the chest, abdomen and pelvis was performed. This confirms the presence of widespread nodular infiltrates throughout both lungs (left-hand pane, lung window) in addition to mediastinal lymphadenopathy (right-hand pane, soft tissue window, arrow) without evidence of primary thoracic or abdominal malignancy. The CT appearances were highly suggestive of disseminated TB which was subsequently confirmed clinically
Cardiac CT – uses ECG gating to acquire and reconstruct imaging data at specific phases of the cardiac cycle (typically during diastole). This enables in most cases motion free images of the coronary arteries to be produced permitting exclusion of obstructive coronary disease or evaluation of aortic disease such as dissection.
Abdomen and pelvis – CT is sensitive in detecting fluid collections, visceral perforation and ischemia. It is particularly useful in the retroperitoneum where ultrasound can be difficult (Fig. 3.5a, b). CT is considered the modality of choice for the assessment of the majority of intra-abdominal pathologies ranging from cases of suspected bowel ischemia (Fig. 3.6), post-operative sepsis (Fig. 3.7a, b) and evaluation of solid organ injury following blunt (Fig. 3.8a, b) and penetrating abdominal trauma.