Chapter 10 Congenital heart disease
Transoesophageal echocardiography
Atrial and ventricular septal defects
Transposition of the great arteries
Major aorto-pulmonary collateral arteries (MAPCAs)
Pulmonary arterial hypertension including Eisenmenger’s syndrome
Congenital heart disease
The phrase ‘congenital heart disease’ encompasses a range of cardiovascular problems from simple patent foramen ovale (PFO) to complex conditions such as tetralogy of Fallot. Cardiovascular imaging is essential in the diagnosis and understanding of congenital heart disease. Many specialists who train in congenital heart disease include a dedicated imaging component in their training.
Cardiovascular imaging
 CMR and transthoracic echocardiography (TTE) are the modalities of choice for the routine assessment and follow-up of patients with congenital heart disease.
CMR and transthoracic echocardiography (TTE) are the modalities of choice for the routine assessment and follow-up of patients with congenital heart disease.
 TTE is fundamental to the assessment of congenital heart disease, particularly in the acute setting and at initial diagnosis, but requires a high level of expertise.
TTE is fundamental to the assessment of congenital heart disease, particularly in the acute setting and at initial diagnosis, but requires a high level of expertise.
 All major centres for congenital heart disease will have access to CMR although studies are time-consuming (30–60min) and any patient with a pacemaker or an implantable cardioverter defibrillator (ICD) is currently excluded from CMR examination.
All major centres for congenital heart disease will have access to CMR although studies are time-consuming (30–60min) and any patient with a pacemaker or an implantable cardioverter defibrillator (ICD) is currently excluded from CMR examination.
 CT has been used in the assessment of congenital heart disease for many years, but predominantly for non-cardiac indications such as CT pulmonary angiography. Any patient who is unable or unwilling to undergo CMR can be assessed by multi-detector CT (MDCT). Although flow data will not be available, most other aspects of a CMR study are available within the MDCT dataset.
CT has been used in the assessment of congenital heart disease for many years, but predominantly for non-cardiac indications such as CT pulmonary angiography. Any patient who is unable or unwilling to undergo CMR can be assessed by multi-detector CT (MDCT). Although flow data will not be available, most other aspects of a CMR study are available within the MDCT dataset.
Chest X-ray
Advantages of chest X-ray
 Widely available
Widely available
 Allows serial comparison
Allows serial comparison
Disadvantages of chest X-ray
 Limited data on intracardiac anatomy
Limited data on intracardiac anatomy
 Two-dimensional with compression of 3D data
Two-dimensional with compression of 3D data
What can chest X-ray tell us?
An important point to check in congenital heart disease is the left and right labels on the CXR! In a normal chest X-ray there will be a left fundal bubble, a left cardiac apex, long left and short right bronchi, and a rightsided liver. Some key signs of congenital heart disease to be aware of are the following.
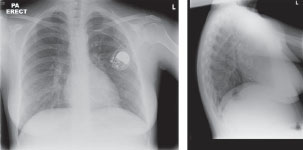
 Situs: fundal bubble (usually left); cardiac apex (usually left), bronchial tree (normally long left, short right), position of liver (Fig. 10.1).
Situs: fundal bubble (usually left); cardiac apex (usually left), bronchial tree (normally long left, short right), position of liver (Fig. 10.1).
 Extracardiac: trachea, cervical ribs, thoracotomy/sternotomy scars, kyphoscoliosis, diaphragms? Raised post-op, clips, prosthetic devices, sternal wires (not always used in paediatric cardiac surgery), pacemaker/ICDs and position of leads, rib notching in aortic coarctation (Fig. 10.2).
Extracardiac: trachea, cervical ribs, thoracotomy/sternotomy scars, kyphoscoliosis, diaphragms? Raised post-op, clips, prosthetic devices, sternal wires (not always used in paediatric cardiac surgery), pacemaker/ICDs and position of leads, rib notching in aortic coarctation (Fig. 10.2).
 Cardiothoracic ratio:?enlarged,?dilated right-side.
Cardiothoracic ratio:?enlarged,?dilated right-side.
 Cardiac silhouette: certain typical patterns.
Cardiac silhouette: certain typical patterns.
 Aortic arch:?collaterals, right-sided arch.
Aortic arch:?collaterals, right-sided arch.
 Calcification of conduits.
Calcification of conduits.
 Pulmonary arteries: dilatation or absence.
Pulmonary arteries: dilatation or absence.
 Lung markings: vascular and parenchyma.
Lung markings: vascular and parenchyma.
 Pleural effusions.
Pleural effusions.
Fig. 10.1 30-year-old female patient with an unoperated secundum atrial septal defect showing dilated right heart, enlarged pulmonary arteries, and pulmonary plethora.

Echocardiography
Advantages of echocardiography
 Portable and widely used non-invasive imaging tool
Portable and widely used non-invasive imaging tool
 Non-invasive detailed anatomical information with serial assessment
Non-invasive detailed anatomical information with serial assessment
 Flow assessment.
Flow assessment.
Disadvantages of echocardiography
 Anatomical knowledge and understanding of congenital heart disease essential when performing echoes
Anatomical knowledge and understanding of congenital heart disease essential when performing echoes
 Studies are operator dependent
Studies are operator dependent
 May be difficult to see some aspects of the cardiac system or vascular connection.
May be difficult to see some aspects of the cardiac system or vascular connection.
What can echocardiography tell us?
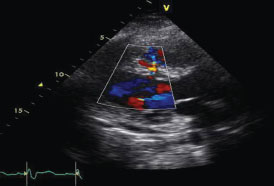
All the basic principles of TTE (assessment of ventricular function, valvular function, and presence of a pericardial effusion) are usually possible in all patients and a full dataset is acquired, including suprasternal, subcostal, and right parasternal views (Figs. 10.3 and 10.4). Some key aspects that are of importance when performing echocardiography in congenital heart disease patients are as follows.
 It is useful to start imaging after you have tried to visualize the anatomy.
It is useful to start imaging after you have tried to visualize the anatomy.
 A sequential segmental approach must be used in all patients.
A sequential segmental approach must be used in all patients.
 Patients may have more than one lesion.
Patients may have more than one lesion.
 Doppler assessment of valves, aortic arch (coarctation), shunt calculation (rarely used), and baffle obstruction (patients who have had arterial switch transposition of the great arteries (TGA)) is possible.
Doppler assessment of valves, aortic arch (coarctation), shunt calculation (rarely used), and baffle obstruction (patients who have had arterial switch transposition of the great arteries (TGA)) is possible.
 Contrast bubble echo can be used for the identification of shunts (e.g. PFO).
Contrast bubble echo can be used for the identification of shunts (e.g. PFO).
 Dobutamine stress echo can be used in patients who have had arterial switch TGA to assess for ischaemia.
Dobutamine stress echo can be used in patients who have had arterial switch TGA to assess for ischaemia.
 Advanced techniques can all be used to derive further information, including tissue Doppler for ventricular function and 3D for detailed anatomical information (e.g. Ebstein’s anomaly, atrioventricular septal defect), speckle tracking, and dyssynchrony assessment.
Advanced techniques can all be used to derive further information, including tissue Doppler for ventricular function and 3D for detailed anatomical information (e.g. Ebstein’s anomaly, atrioventricular septal defect), speckle tracking, and dyssynchrony assessment.
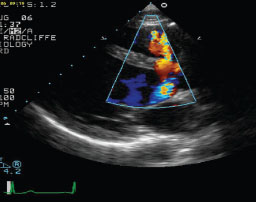
Fig. 10.3 Parasternal long-axis view with TTE demonstrating a perimembranous ventricular septal defect (VSD). Colour flow mapping shows the jet between the left ventricular outflow tract and the right ventricle. In this situation it is important to assess the aortic valve and identify any aortic regurgitation.
Transoesophageal echocardiography
What can TOE tell us?
Experience is essential for interpreting TOE in complex CHD and therefore should be undertaken in specialist centres and/or by specialists in congenital heart disease. TOE is usually used perioperatively to assess patients before and during the procedure. This is the case for both surgical and percutaneous procedures (ASD/PFO/VSD closure, valve surgery) (Fig. 10.5). Increasingly 3D TOE is being used to allow better visualization of variation in the 3D cardiac anatomy.
Two things to be aware of in patients with congenital heart disease are as follows:
 care should be taken with sedation as this may result in cardiovascular collapse
care should be taken with sedation as this may result in cardiovascular collapse
 always check for previous oesophageal surgery or abnormalities.
always check for previous oesophageal surgery or abnormalities.
A sequential analysis is used and some of the particular areas of the cardiovascular system that lend themselves to evaluation by TOE are:
 pulmonary veins
pulmonary veins
 pathways/baffles/communications/intracardiac thrombus (prior to cardioversion)
pathways/baffles/communications/intracardiac thrombus (prior to cardioversion)
 contrast/bubble echo to identify shunts/PFO
contrast/bubble echo to identify shunts/PFO
 assessment of endocarditis
assessment of endocarditis
 assessments of aorta such as patent ductus arteriosus (PDA), coarctation, outflow tract obstruction
assessments of aorta such as patent ductus arteriosus (PDA), coarctation, outflow tract obstruction
 patients with difficult transthoracic views (e.g. chest deformity)
patients with difficult transthoracic views (e.g. chest deformity)
 ventricular function from transgastric views in patients with difficult views.
ventricular function from transgastric views in patients with difficult views.
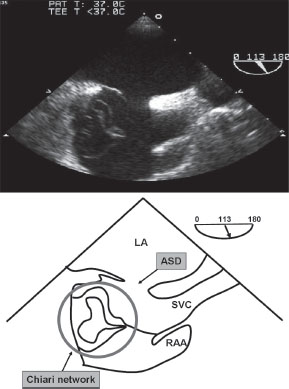
Fig. 10.5 Transoesophageal bicaval view demonstrating a secundum atrial septal defect. A Chiari network with multiple stands of the network extending across the right atrium is also evident.
Cardiac magnetic resonance
Advantages of CMR
 Any imaging plane is possible.
Any imaging plane is possible.
 Independent of body habitus.
Independent of body habitus.
 Accurate quantification of cardiac chambers.
Accurate quantification of cardiac chambers.
 Can assess vasculature and aorta as well as heart.
Can assess vasculature and aorta as well as heart.
 Can study chest and other areas of body during the same study.
Can study chest and other areas of body during the same study.
Disadvantages of CMR
 Specialist experience in both congenital heart disease and CMR are essential during acquisition (to ensure that the correct sequences are recorded) and interpretation scan. Therefore congenital CMRs are usually only undertaken in specialist centres.
Specialist experience in both congenital heart disease and CMR are essential during acquisition (to ensure that the correct sequences are recorded) and interpretation scan. Therefore congenital CMRs are usually only undertaken in specialist centres.
 Expensive and limited availability.
Expensive and limited availability.
 Potentially lengthy scans with long breath-holds.
Potentially lengthy scans with long breath-holds.
 Susceptibility to artefacts from stents, sternal wires, and rods from spinal deformity surgery.
Susceptibility to artefacts from stents, sternal wires, and rods from spinal deformity surgery.
 Pacemakers, ICDS, metallic implants, and aneurysm clips are contraindicated.
Pacemakers, ICDS, metallic implants, and aneurysm clips are contraindicated.
 Some patients are claustrophobic (2%).
Some patients are claustrophobic (2%).
What can CMR tell us?
CMR is a standard cardiovascular investigation for assessment of congenital heart disease. It is particularly useful for the following.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


