CHAPTER 11 Contrast Agents and Medications in Cardiac Computed Tomography
Earlier generations of multidetector CT scanners provided the foundation for cardiac multidetector CT angiography, and the implementation of 64-multidetector CT technologies made it a reliable tool with a high degree of diagnostic efficacy.1–3 In contrast to CT angiography applications using intravenous contrast medium (CM) administration elsewhere in the body, adequate cardiac opacification is not always simple to achieve, particularly in light of continuously evolving CT technology, with scan times becoming substantially shorter, but yielding improved spatial and temporal resolution. Empiric injection protocols are no longer adequate because they do not take into account the complexity of all confounding variables that allow consistent, robust cardiac imaging.4 These confounding variables include the requirement for a controlled and regular heart rate and carefully timed arterial enhancement for optimal cardiac and coronary vessel enhancement during minimal cardiac motion. Physiologic and pharmacokinetic constraints of cardiac enhancement in addition to inherent technical scanner properties have to be considered when building an integrated scanning and injection protocol for cardiac CT angiography.
TECHNICAL REQUIREMENTS
Medications for Cardiac Imaging
Although newer generations of multidetector CT scanners have shown a substantial improvement in temporal resolution—and with this, the capability to “freeze” cardiac motion—it is still desirable for most cardiac applications to slow the heart rate for various reasons. Slow heart rates prolong the cardiac phases with the least cardiac motion, specifically end-diastolic relaxation and end-systolic contraction. Best image quality is achieved when the data reconstruction window fits temporally into these phases.5 Slower heart rates also decrease heart rate variability during data acquisition and allow optimal efficacy of ECG-gated dose modulation techniques to control patient radiation dose.6
In our practice, we aim for a target heart rate less than 65 beats/min. To slow the heart rate, β blockers are ubiquitously used, and different means of β blocker administration for cardiac imaging are described, depending on patient, workflow, and logistics-related factors. Knowledge of the pharmacologic properties of the various β blockers is key to ensure safe and efficient patient prescan preparation. First-generation agents, such as propranolol, nonselectively block all β receptors (β1 and β2 receptors). Second-generation agents, such as atenolol, metoprolol, acebutolol, and others, have a relative selectivity, when given in low doses, for β1 (largely cardiac) receptors. The administration of β1 adrenoreceptor antagonists is favored for cardiac CT because of fewer side effects and fewer contraindications. Table 11-1 summarizes the effects mediated by β1 and β2 adrenoreceptors, and Figure 11-1 shows the important effects of nonselective and selective β blockers.
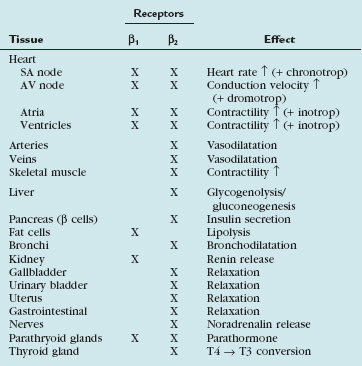
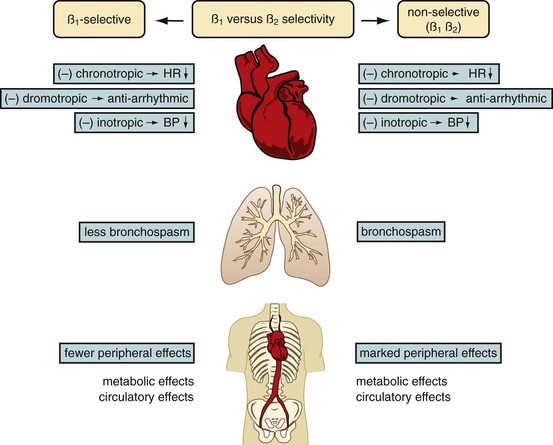
 FIGURE 11-1
FIGURE 11-1Diverse cardiac CT imaging centers have proposed different protocols of β blocker administration. Some centers routinely use an oral β blocker (e.g., atenolol [Tenormin]) to slow the heart rate and add an intravenous β blocker (e.g., metoprolol tartrate [Lopressor]) only if rate control is unsatisfactory. Other centers performing cardiac CT suggest different medication protocols (i.e., no combination of intravenous and oral β blocker administration) based on their experience and available operational logistics. Table 11-2 shows the sequence of our routine β blocker administration in the absence of any contraindications. Any patient preparation protocol should include a checklist for contraindications to the use of β blockade. The general contraindications for the therapeutic use of β blockers also apply for a “one-time” use for cardiac CT. Table 11-3 summarizes the most important contraindications for the drugs involved in cardiac CT. In case of questionable contraindications, the responsible imaging specialist should confer with the referring physician and determine if the administration of a β blocker is justified, or if alternatives should be applied.
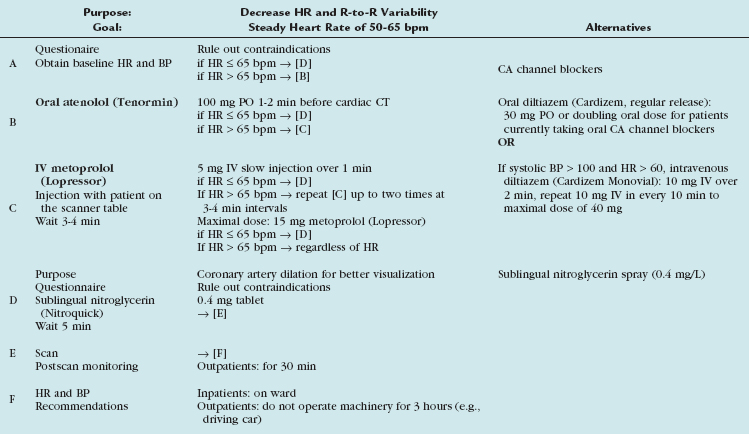
Table 11-3 Contraindications for the Use of β Blocker, CA Channel Blockers, and Nitroglycerin for Cardiac CT
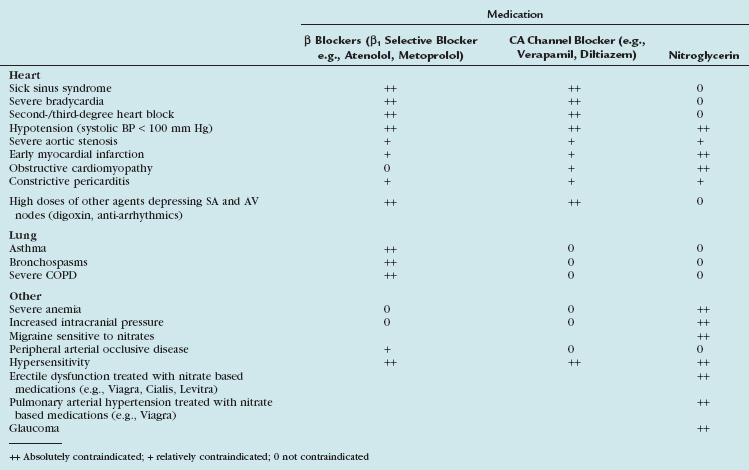
Calcium channel blockers embody an alternative heart rate-controlling medication. In patients with contraindications to β blockers (i.e., asthma), an attempt with calcium channel blockers may be worthwhile. There is less experience with calcium channel blockers in the setting of cardiac CT, and the imaging physician should be familiar with the medication, its administration (see Table 11-2), and its contraindications (see Table 11-3). Consultation with the referring physician is suggested to obtain an optimal and safe result.
Organic nitrates are widely used to treat angina and alleviate symptoms of myocardial ischemia through various mechanisms.7 Intracoronary injection of nitroglycerin has long been used to obtain maximal arterial dilation during conventional coronary angiography.8 Similarly, oral administration of short-acting nitrates (sublingual nitroglycerin tablets or sublingual nitroglycerin spray) is an accepted practice to dilate the lumen of the coronary arteries during coronary CT angiography.9 Its vasodilative effect on the coronary arterial bed allows improved visualization of smaller arterial branches.10 The significant impact on the diameter of coronary arteries seems to be more pronounced in nondiseased/nonstenotic coronary segments when compared with diseased/stenotic coronary segments.11 This additional pharmacologic end-organ response is a welcome side effect because it accentuates further the difference between diseased and nondiseased coronary segments, and improves depiction of subtle coronary arterial disease. In addition to dilation of the vascular bed, nitroglycerin suppresses potential coronary artery spasm that may mimic stenosis at coronary CT angiography, especially in younger patients.
Our rationale of nitroglycerin administration is summarized in Table 11-2. Because the blood level peaks around 2 minutes, and the half life is around 7 minutes, we suggest waiting approximately 5 minutes after sublingual nitroglycerin administration to ensure maximal effect of coronary artery vasodilation.
The side effects of nitroglycerin are harmful; severe decreases in blood pressure and death have been reported in patients given nitroglycerin within 24 hours because of a pharmacologic interaction with phosphodiesterase type 5 inhibitors (e.g., sildenafil citrate [Viagra] or tadalafil [Cialis]). A careful check for any contraindications before administration of nitroglycerin must be a part of any patient premedication protocol (see Table 11-3).
Contrast Media
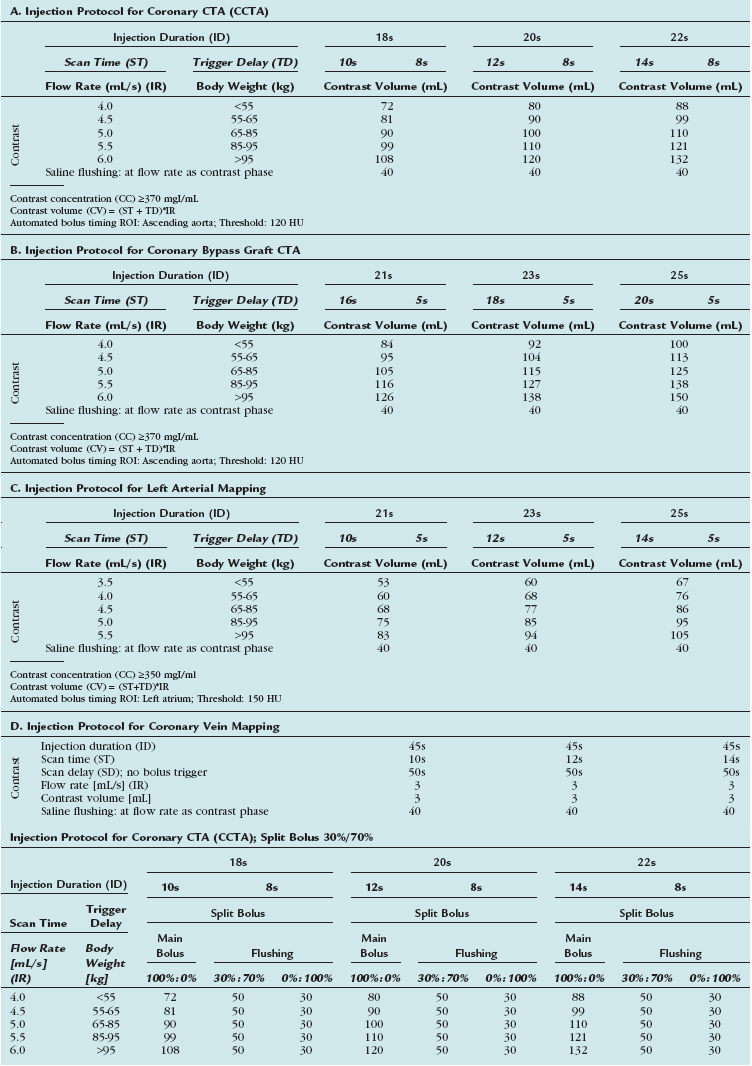
CT contrast agents are water-soluble derivates of iodinated benzene rings, which are either charged (ionic contrast agent) or not charged (nonionic contrast agent) monomeric or dimeric chemical structures. The x-ray absorption is proportional to the concentration of the iodine captured within the agent.12 Other important physicochemical properties of CM are their osmolality (high-osmolar, low-osmolar, iso-osmolar) and viscosity. Higher flow rates are necessary for cardiac CT imaging. Warming the contrast agent to body temperature reduces viscosity and maintains high injection flow rates.13 The viscosity of CM decreases about 50% by heating it from 20° C to body temperature.
Safety Issues of Contrast Media
Nonionic contrast agents for CT angiography are considered to be very safe with an adverse event rate of approximately 3%.14 Most adverse effects are mild to moderate, but severe reactions may occur in approximately 0.04%.15 Non–dose-dependent, (idiosyncratic) allergy-like and dose-dependent (nonidiosyncratic) reactions are the two major categories of adverse effects. Guidelines for patient screening, premedication, and management of acute adverse reactions are available in the literature.16 There is also a substantial incidence of delayed cutaneous reactions occurring 24 hours or more after CM injection.17 Because these events tend to recur with reinjection of the same CM, screening and documentation of these reactions is of paramount importance.17 Another absolute contraindication for iodinated CM is manifest hyperthyroidism (i.e., Graves disease) with the risk of triggering a thyrotoxic crisis.18
Important dose-dependent effects include CM extravasation, cardiovascular effects, drug interactions, and contrast-induced nephropathy (CIN). CM extravasation is a well-known problem that occurs with an incidence of approximately 0.2% to 0.6% with the use of mechanical power injectors.19 Injection flow rates of 5 to 6 mL/s are routinely used for cardiac CT imaging and are considered to be safe.20 Only large volumes (>30 mL) of CM extravasation are at risk of severe side effects such as skin necrosis, ulceration, or compartment syndrome. Although adverse effects are more common and severe with ionic CM, they have been described to occur occasionally with nonionic agents as well. Conservative management of extravasation injuries (applying warm or cold compresses) is often adequate. For more severe injuries, plastic or hand surgery consultation is recommended to determine optimal treatment. Any adverse effects should be documented for future therapeutic planning.
To avoid any extravasation, intravenous access should be tested for stable and correct cannula position by a preliminary rapid manual injection of saline with the patient’s arm in the scanning position. Most extravasation events happen within the first seconds of injection; however, they may also occur later during mid or late phase of injection. Checking the intravenous access during early CM administration does not entirely prevent any extravasation. Extravasation detection devices linked to the power injector provide monitoring during the entire CM administration and may reduce the risk of late extravasation.21 Their use comes, however, with increased cost and risk of erroneous abortion of CM administration because of false-positive alarms.
Cardiovascular adverse events after intravenous administration of nonionic agents are probably rare; the literature suggests that severe reactions are more likely to be due to cardiopulmonary decompensation than to allergy-like reactions.22 Rapid injection of CM volume may lead to acute decompensation in patients with preexisting substantial cardiopulmonary compromise. Reducing the CM volume and injection rate seems to be one rational technique to reduce this specific risk.
CIN resulting from nonionic CM is rare (<2%) in the general population, but it may be substantial in the subset of patients at increased risk (>25%).23 CIN is defined as a greater than 25% increase of serum creatinine from baseline value within 3 days after CM injection in the absence of other causes.24 Controversy exists currently as to which features of the CM abet the development of CIN. In most cases, CIN is reversible, but it may be associated with considerable morbidity and mortality.25
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


