Conventional radiographic imaging remains an important tool in the era of cross sectional imaging, particularly in the pediatric population. In this chapter we revisit the importance of plain ‘scout’ films before reviewing the array of fluoroscopic imaging technologies used for imaging the pediatric genitourinary tract. For the pediatric population, the concept of ALARA (as low as reasonably achievable) and ‘image gently and step lightly’ needs to be followed to minimise radiation exposure.
The scout film – is it really necessary?
The American College of Radiology (ACR) practice guidelines state: ‘If a recent abdominal image is not available, a preliminary abdominal radiograph, fluoroscopic image capture, or digitally acquired spot image may be obtained before instilling contrast media in order to detect opaque calculi or other calcifications and to evaluate anatomy such as skeletal anomalies. A digitally acquired spot image or radiograph may be preferable to fluoroscopic image capture in specific clinical situations needing superior spatial resolution’. This image also allows for detection of intraabdominal contrast material from a recent examination, which would confound further interpretation.
Radiographic procedures like IVU (intravenous urography), MCU (micturating cystourethrogram)/VCUG (voiding cystourethrogram), RGU (retrograde urogram) are often performed in cases where ultrasound revels unilateral/bilateral urinary tract dilatation particularly of the calyces and ureters, signs of urethral obstruction especially with those neonates where antenatally diagnosed genitourinary anomalies have been documented.
These procedures are performed under planned fluoroscopic guidance such that the radiation doses are not significant. Just like any other investigation, the goal is to minimise radiation dose and maximise the information obtained and the same has been stresses upon by ALARA principle.
Normal hepatic and splenic soft tissue density can be appreciated in both upper quadrants. The properitoneal fat strip can be seen in bilateral paracolic gutters and the psoas and renal shadows can also be appreciated (Fig. 10.6.1).
Fig. 10.6.1Normal plain scout image showing soft tissue density outlines of liver (L), spleen (S), kidneys (R) and psoas shadow (dotted line).
Various abdominal calcifications can be seen on the scout film and need to be differentiated from renal calcifications. They include gallbladder calculi which appear as multiple faceted calcifications in the right upper quadrant, calcific chronic pancreatitis which is seen as multiple stippled calcifications in the upper abdomen adjacent to the lumbar spine, adrenal or hepatic calcifications appear as stippled and discrete calcifications overlying the right twelfth rib. Renal calculus is seen as separate deposits of calcified density confined to the renal shadow. Other calcifications within the renal shadow include cortical and medullary nephrocalcinosis (Figs. 10.6.2 and 10.6.3). Stippled suprarenal calcification in a paediatric patient may point towards a neuroblastoma while rim calcification may be seen in a case of adrenal haemorrhage (Fig. 10.6.4). Calcifications seen in the pelvis can point towards a bladder calculus, ureteric calculus, phlebolith or an intrauterine copper device, calcified fibroid or dermoid cyst in a female patient.
Fig. 10.6.2Diffuse calcification of bilateral renal cortices suggestive of cortical nephrocalcinosis. It can be associated with chronic glomerulonephritis, shock, sepsis, chronic pyelonephritis etc.
Fig. 10.6.3Deposition of calcium salts in the medulla of the kidney suggestive of medullary nephrocalcinosis. It can be associated with hyperparathyroidism, medullary sponge kidney, renal tubular acidosis (type 1), hypervitaminosis D, milk-alkali syndrome etc.
Fig. 10.6.4A well-defined rounded lesion with peripheral rim calcification in the right hypochondrium in an infant with perinatal adrenal haemorrhage which has now calcified.
Skeletal abnormalities like spina bifida, lumbar vertebral anomalies, osteoporotic changes, looser zones and bone tumours can also be seen on the plain radiograph. The association of skeletal anomalies such as spina bifida, caudal regression, and wide pubic symphysis may help in further defining associated syndromic criteria.
Features suggestive of secondary hyperparathyroidism like medullary nephrocalcinosis, rugger jersey spine, subchondral bone resorption around the sacroiliac joints, subtendinous bone resorption at ischial tuberosity and dystrophic soft tissue calcification can also be seen.
Micturating/voiding cystourethrogram
The most common indication for a fluoroscopic MCU/VCUG is the evaluation of urinary tract infection (UTI). Voiding dysfunction, enuresis and work-up for antenatally diagnosed hydronephrosis are other indications. Presence or absence of VUR, as well as anatomic abnormalities of the bladder and urethra, can be diagnosed by MCU.
Procedure
Educating and informing the parent about the procedure is necessary as it involves urethral catheterization.
No sedation is required for this procedure. A real-time fluoroscopic examination is performed. Urethral catheterization is done under sterile conditions on the fluoroscopy table. A 5-F feeding tube is appropriate in children under 3 months of age and an 8-F feeding tube in all other children.
Precontrast scout – Evaluate for calcifications and assess bowel pattern. Catheter position is also documented on this scan.
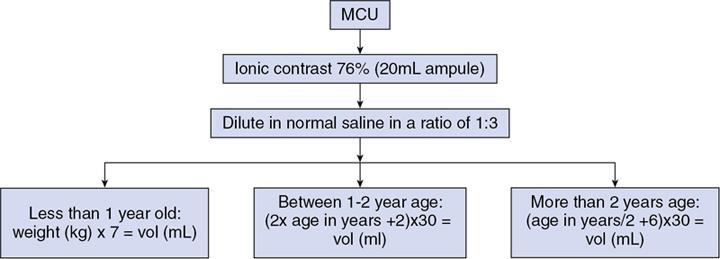
Low iodine concentration (approx. 25% weight/volume) contrast agent (Meglumine Diatrizoate), is taken to fill the bladder, typical 20 mL in an infant to 500 mL in an adult. Contrast is then dripped from a height of no greater than 60 cm (physiological filling pressure of 30–40 cm water). Rapid bladder filling using a syringe may generate high pressures leading to bladder distension and artificial VUR, as well as altered bladder capacity values. Normal bladder capacity increases during the first 8 years of life, and bladder capacity for a child less than 8 years can be calculated as (age [years] + 2) × 30 (Fig. 10.6.5).
Postcontrast views
Early filling view of bladder – within few seconds of contrast instillation and AP view is taken. This helps to rule out an ureterocele which is seen as a round, well-defined filling defect. These can be compressed and get obscured on late filling films (Fig. 10.6.6).
Intermediate filling phase – not recommended. In order to assess the minimum bladder volume beyond which reflux occur or to assess the amount of ureteral reflux, nuclear cystography is recommended which will also have a prognostic importance.
Filled view of bladder and VUJ – preferably bilateral oblique views of a full bladder to visualize the VUJs. This can be done by positioning the bladder at the inferior most part of screen and tilting the tube along the course of the ureter. Abnormalities of the bladder like congenital or acquired bladder diverticula, patent urachus can be diagnosed on this image (Figs. 10.6.7 and 10.6.8). Conditions like pelvic lipomatosis can also be diagnosed by appreciating the ‘pear shaped’ bladder. An anteroposterior imaging of the renal fossa can be done prior to voiding in case reflux is detected in the late bladder filling phase. To follow the principle of ALARA and Image Gently, while imaging female patients, spot radiographs of the renal fossa should be centred on the fossa not including the region of the gonads or the urine-filled bladder.
Voiding urethra view
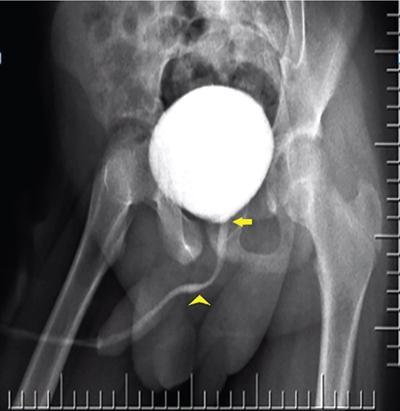
Male patient – steep oblique position is optimum (Fig. 10.6.9).
Female patient – anteroposterior view is preferred which will show a classical spinning top appearance (Fig. 10.6.10).
This image will depict abnormalities of the posterior urethra like posterior urethral valve, outlet obstruction as well as point towards a possible VUR (Fig. 10.6.11). One image can be obtained with the catheter in situ and another with the catheter removed. Voiding with catheter in situ allows refilling if needed and drain bladder in patients who are unable to void completely. A neurologic abnormality, bladder spasm or active bladder infection can be indicated by low voiding volumes. However, reproducibility of these findings should be documented for this observation to be reliable. An unexpectedly large bladder capacity may be seen in sensitive voiders, dysfunctional voiding or noncompliant recently trained children. May be due to noncompliance in recently toilet-trained children.
Cyclical voiding – this increases detection of VUR significantly. Second-cycle voids can also increase the grade of reflux that was detected on the first void.
Kidneys and pelvis – this is the most important view to demonstrate VUR. In a patient with VUR reflux will be seen in the ureters and/or the kidneys depending upon the grade (Figs. 10.6.12 and 10.6.13A–D). Fifteen-minute delayed abdominal imaging after voiding can help in differentiating simple reflux from reflux associated with obstruction at the ureteropelvic or ureterovesical junction. Certain conditions like ureteral duplication, prune belly, bladder diverticula, posterior urethral valves can coexist with VUR. The use of fluoroscopy should be brief and intermittent during bladder filling.
Fig. 10.6.5Calculation of contrast volume for MCU study according to age.
Fig. 10.6.6Well-defined round filling defect is seen in the urinary bladder on the left side consistent with a left ureterocele.
Fig. 10.6.7Patent urachal diverticulum can be seen in the filled bladder view as a tubular outpouching arising from the dome of the bladder towards the umbilicus.
Fig. 10.6.8A sinogram performed through the umbilical opening of a patent urachal sinus.
Fig. 10.6.9Normal appearance of a male urethra on an MCU. Yellow arrow points towards the prostatic urethra. The bulbar portion is marked by the arrowhead. Between the two lies the membranous urethra and distal to the bulbar urethra lies the penile urethra.
Only gold members can continue reading. Log In or Register to continue