This review proposes a structured approach to analyzing conventional radiographs of adult hips by focusing on alterations of radiological bone density, femoral head contours, and the joint space. Conventional radiography enables detecting subtle changes in cortical contours and joint space width due to its high spatial resolution. It is limited to the detection of cortical changes in areas to which the x-ray beam is tangent. It has reduced sensitivity for the detection of trabecular bone and medullary changes. Radiographic findings in common hip disorders, such as osteoarthritis, osteonecrosis, transient osteoporosis, and subchondral insufficiency fractures, are correlated to changes on MR imaging and computed tomography.
Key points
- •
Conventional radiographs continue to play an important role in the first-line evaluation of symptomatic hip joints despite the advent of MR imaging.
- •
Comparative anteroposterior and off-lateral views of the hips enable an accurate evaluation of the joint space.
- •
Radiographs have limited sensitivity in detecting bone changes.
- •
Radiographs cannot detect joint effusion and bone marrow changes.
Introduction
Conventional radiography is frequently used as the initial imaging modality to assess hip disorders. The aim of this review article is to provide a structured approach to analyze conventional radiography of normal and abnormal adult hips. We will focus on changes in radiological bone density and contours of the femoral head and alterations of the joint space observed in common hip disorders, which include osteoarthritis, femoral head osteonecrosis, transient osteoporosis, and subchondral insufficiency fractures. The findings at radiography are correlated with MR imaging and computed tomography (CT). Pediatric, metabolic, neoplastic, and postoperative hip disorders will not be addressed. Conditions in which correlation with cross-sectional imaging does not bring added value for the understanding of conventional radiography will be out of the scope of this review.
Anatomy of the hip and challenges in hip disorders
The hip is a deeply located highly congruent diarthrodial joint. A nearly spherical femoral head articulates with the acetabular cavity, which is reinforced by an acetabular labrum, and the capsular ligaments (the medial and lateral arms of the iliofemoral ligament, the pubofemoral ligament, and the ischiofemoral ligament) ( Fig. 1 ). Hip radiographs only demonstrate bone contours to which the x-ray beam is tangent ( Fig. 2 ).

Medical imaging plays a major role in the work-up of patients with suspected hip disorders because the deeply located hip is not amenable to direct palpation and the clinical examination may be restricted to evaluating the range of motion.
Radiological work-up of the hip
Radiological work-up of the hip includes an anteroposterior (AP) radiograph of the pelvis and a lateral radiograph of the symptomatic hip. The pelvic radiograph allows the assessment of the entire pelvic girdle, providing an overview of the entire region. Moreover, by allowing the comparative analysis of both hips, it enhances the detection of subtle bone and joint abnormalities. The AP pelvic radiograph should be obtained with the patient lying supine, the lower limbs medially rotated (20 degrees). When obtained in a standing position, it enables detecting leg length discrepancy but provides a less satisfactory analysis of the bone structure. Standing hip radiograph does not provide additional information on the joint space except in severe hip dysplasias, opposite to the knee joint, for which proper assessment of the joint space width requires weight-bearing radiographs.
The added value of an AP hip radiograph to complement pelvic radiograph is open to debate except after total hip replacement. In the authors’ institution, an AP hip radiograph usually is obtained because of the high quality of the bony details secondary to beam collimation. Several different lateral views of the hip can be obtained, the choice of which may depend on the clinical situation ( Fig. 3 , Table 1 ). Most of the lateral radiographs are obtained with different degrees of hip abduction and flexion providing a lateral view of the proximal femur. The off-lateral view (also called false profile of Lequesne) is a unique radiograph that provides an evaluation of the hip joint in a near sagittal plane, with the femur in an anatomic position ( Fig. 4 ). It allows analyzing the most anterior and posterior aspects of the joint space that are not depicted on the AP and the other lateral radiographs, at the expense of a decrease in the overall quality of the image.

| Radiographic Projection | Value | Limitation | Common Indication |
|---|---|---|---|
| Off lateral view (Lequesne false profile) |
| Poor evaluation of the femoral neck |
|
| Lateral both hips (frog-leg projection) |
|
|
|
| 45° posterior oblique, (Lauenstein projection) |
|
| |
| 30° anterior oblique (Judet projection) |
|
|
|
| True lateral neck of femur (cross-table lateral view) |
|
|
|
| Urethral profile |
|
|
|
| Dunn profile |
|
|
|

Conventional radiography yields a high spatial resolution that enables detecting subtle changes in cortical contours and joint space width. Because conventional radiography corresponds to a bidimensional projection of 3-D structures, however, it can only detect cortical changes to which the x-ray beam is tangent (see Figs. 1 and 4 ). Other limitations of conventional radiography of the hip include limited sensitivity for the detection of trabecular bone and medullary changes and the inability to show joint effusion ( Fig. 5 ).

Radiological density of the femoral head
Normal Radiological Density of the Femoral Head
The physician interpreting conventional hip radiographs should first focus on alterations in radiological bone density. The radiographic appearance of the hip joint is largely influenced by its anatomy. The femoral head varies in thickness due to its spherical shape and it contains a thin sclerotic line that corresponds to the remnant of the physis (also called the physeal scar). The head is partially covered by the acetabulum, which is obliquely oriented in the coronal and axial planes. The radiological density of the femoral head can be divided into 3 zones, reflecting the superimposition of the anterior and posterior acetabular walls and their oblique orientation ( Fig. 6 ). The upper medial zone shows the highest bone density due to the superimposition of both acetabular walls on the upper femoral head. It is delimited by the upper limit of the femoral head superiorly and the anterior acetabular wall inferiorly. The intermediate zone shows intermediate density and is delineated by the projection of the anterior acetabulum medially and by the posterior acetabulum laterally. The lower and lateral zone of the femoral head shows the lowest density and corresponds to the lateral aspect of the femoral head projecting outside the acetabular borders. The relative importance of these 3 zones is largely dependent on the anatomy and the position of the body relative to the direction of the x-ray beam. Any deviation from this normal zonal description may reflect an alteration of the bone density, the only exception being the physeal scar. The apparent radiological density of the femoral head also may depend on technical factors, acetabular changes and other superimposing structures.

Increased Radiological Density of the Femoral Head
Femoral head osteonecrosis
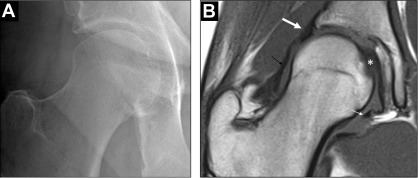
Femoral head osteonecrosis can be associated with increased radiological density of the femoral head ( Table 2 ). Bone hyperostosis is mainly due to trabecular bone apposition at the margin of or within the osteonecrotic lesion. Therefore, the radiological hallmark of osteonecrosis is the presence of a sharply delineated sclerotic lesion in the femoral head that represents the sclerotic interface that separates the subchondral necrotic segment of the epiphysis from the normal adjacent bone when the x-ray beam is tangent to it ( Fig. 7 ). Occasionally, the sclerotic zone may appear ill defined, without sclerotic line, on the AP radiograph. The sclerotic bone margin may become more conspicuous on the oblique projection of the femoral head ( Fig. 8 ). When the lesion is extensive it may involve the entire femoral head with a horseshoe pattern and it becomes difficult to detect the real margins of the necrotic lesion on the radiographs ( Fig. 9 ).
| Examples | Histologic Correlation | Radiological Features |
|---|---|---|
| Osteoarthritis |
|
|
| Femoral head osteonecrosis |
|
|
| Subchondral insufficiency fracture |
|
|



Subchondral insufficiency fracture
In patients with subchondral insufficiency fracture, a subtle increase in bone density in the subchondral area can be observed, usually late in the course of the disease ( Fig. 10 ). These subtle sclerotic changes are probably due to callus formation in the subchondral area.

Osteoarthritis
In advanced hip osteoarthritis, increased radiological bone density can be seen in association with important joint space narrowing. These changes, related to the thickening of the subchondral bone plate and/or of the trabecular bone network, can occur on either or both sides of the joint ( Fig. 11 ).

Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


