| SKULL BASE REGION | Sellar/suprasellar |
| HISTOPATHOLOGY | Craniopharyngioma, adamantinomatous type |
| PRIOR SURGICAL RESECTION | Yes |
| PERTINENT LABORATORY FINDINGS | Low thyroid stimulating hormone/T3/T4, low growth hormone/insulin-like growth factor-1 |
Case description
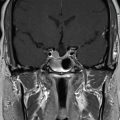
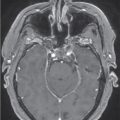
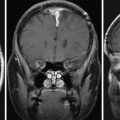
The patient is a 16-year-old male who was evaluated for delayed growth and pubertal development. He was initially diagnosed with hypothyroidism and started on levothyroxine, followed by growth hormone injections 1 year later, after which he gained 10 inches in height. Six months later, the patient developed diplopia, progressive loss of peripheral vision, and bitemporal hemianopia confirmed on Goldmann visual fields testing. Brain magnetic resonance imaging (MRI) revealed a large heterogeneous solid and cystic sellar mass extending superiorly into the third ventricle and compressing the optic chiasm ( Figure 4.16.1 ). He underwent transsphenoidal resection of the tumor and reconstruction with a nasoseptal flap. Gross total resection (GTR) was achieved ( Figure 4.16.2 ), and pathology confirmed a WHO grade I craniopharyngioma, adamantinomatous type. Following surgery, the patient’s vision normalized; however, he developed diabetes insipidus that was managed with desmopressin (DDAVP). The patient also required long-term replacement of testosterone, hydrocortisone, and levothyroxine, but the growth hormone replacement was discontinued. A year later, he developed a collapsed nasal septum with saddle nose deformity and nasal obstruction, for which he underwent surgical correction.


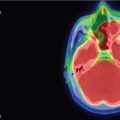
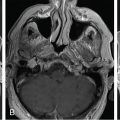
Interval imaging at 16 months post-GTR showed 2 small areas of recurrence in the inferior aspect of the sella ( Figure 4.16.3 ). Stereotactic radiosurgery (SRS) with CyberKnife was recommended, and 2400 cGy was delivered in 1 fraction, which was prescribed to the 80% isodose curve covering the periphery of the inferior sella with a volume of 0.192 cm 3 ( Figure 4.16.4 ).
| Radiosurgery Machine | CyberKnife |
| Radiosurgery Dose (Gy) | 24, at the 80% isodose line |
| Number of Fractions | 1 |

Related posts:
 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
Chordoma – immediate postoperative/post-proton therapy radiosurgery for residual disease
 Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
Trigeminal neuralgia due to microvascular conflict – upfront radiosurgery
 Capillary hemangioma – postoperative radiosurgery for residual tumor
Capillary hemangioma – postoperative radiosurgery for residual tumor
 Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


