(1)
Department of Clinical Radiology, Amiri Hospital – Kuwait City, Kuwait City, Kuwait
8.1 Scleroderma (Systemic Sclerosis)
Scleroderma is a systemic disease characterized by progressive fibrosis of the skin and multiple organs. The term “scleroderma” means literally “hard skin.”
In scleroderma, the dermis is infiltrated by T lymphocytes, causing abnormal fibroblasts activation, which leads to increased production of extracellular collagen type I. This increase in collagen causes skin thickening and tightening, which is the main manifestation of this disease.
Scleroderma is divided into two major forms: diffuse and focal. In the generalized form, diffuse skin disease with organ involvement is typically seen. In the focal form, there is limited cutaneous involvement of the skin. Linear scleroderma and morphea are examples of focal scleroderma.
Females are affected by scleroderma seven times as often as males. Patients present classically with flexural contracture of the terminal phalanges (claw-hand like appearance), loss of the skin folds around the mouth (masklike appearance), atrophied nasal alae (mouse facies), reduced opening of the mouth with jaw fixation, pathological changes of minor salivary glands mimicking Sjögren’s syndrome, and uncommonly trigeminal neuralgia (4 %). Laboratory investigations show positive antinuclear antibodies (70–90 %), rheumatoid factor (25 %), and hyperglobulinemia.
CREST syndrome is a variant of diffuse scleroderma characterized by Calcinosis cutis, Raynaud’s phenomenon, Esophageal dysmotility with dysphagia, Sclerodactyly, and Telangiectasia. Calcinosis cutis is deposition of calcium in the skin producing hard cutaneous nodules. Raynaud’s phenomenon is a series of finger discoloration after exposure to either temperature alternation or emotional disturbance. First, fingers become pale (white) due to small vessels vasoconstriction, then turn blue as the vessels dilate to keep blood flow, and finally turn red as blood flow returns (Fig. 8.1.1). Sclerodactyly means skin thickening of the fingers and toes that produces claw-hand deformity. Telangiectasia is dilatation of the small vessels over the skin and the mucus membranes ranging between 0.51 mm in diameter. They are commonly seen over the face and the neck as small red marks on the skin.

Fig. 8.1.1
An illustration demonstrates the finger discoloration stages of Raynaud’s phenomenon: (a) normal fingers, (b) pale fingers, (c) bluish discoloration due to ischemia, and (d) reddish discoloration due to postischemic hyperemia
Morphea is a superficial-localized form of scleroderma characterized by a plaque of thickened skin, often with an active, violaceous border with a yellow to white center. It is commonly seen in children, with an incidence of 1 per 100,000 individuals. Generalized morphea is a term used to describe morphea lesions covering >30 % of the body surface. Disabling pansclerotic morphea (deep morphea) is a term used to describe morphea that extends deep into the soft tissues with fixation to the underlying structures.
Nodular (keloid) scleroderma is a rare form of cutaneous scleroderma that can occur in association with diffuse scleroderma or morphea. It is seen as keloidal hyperpigmented papules that develop early in the course of the disease. An inflammatory infiltrate is present during the period of active fibrosis.
Linear scleroderma, also known as en coup de sabre, is a localized form of scleroderma seen as a linear, ivory-colored, deforming depression on the scalp and the forehead mimicking a blow of a sword, which is described as “coup de sabre” (Fig. 8.1.2). The lesion usually results in furrowing of the forehead, causing significant facial asymmetry and cosmetic deformity. Linear scleroderma lesions can be seen following Blaschko’s lines (Fig. 8.1.3). These lines determine the distribution of many congenital and acquired skin diseases (e.g., epidermal nevi). Many authors believe that these lines represent the pattern of embryonic migration of skin cells.


Fig. 8.1.2
An illustration demonstrates linear scleroderma affecting the left forehead
Fig. 8.1.3
An illustration demonstrates Blaschko lines over the right forehead. The same lines can be found on the left side
Linear scleroderma is usually seen in children and in the young population, and it can affect the limbs, especially the lower limbs, resulting in unilateral, atrophic limb. Linear scleroderma is usually confused with Parry–Romberg syndrome when it extensively affects half of the face. Brain involvement in linear scleroderma usually presents in the form of epilepsy, with or without brain abnormalities.
Differential Diagnoses and Related Diseases
Hypothenar hammer syndrome (HHS) is a rare condition characterized by episodic digital ischemia as a result of occlusion of the distal ulnar artery at the level of the hamate bone, typically due to repetitive blunt trauma to the ulnar artery at the hypothenar eminence. The ulnar injury usually results from thrombosis or aneurysms from the repetitive trauma. The distal ulnar artery is most vulnerable to trauma at the level of the hook of the hamate, which works as an anvil against the distal ulnar artery as the patient uses his/her hypothenar eminence of the hand. The disease usually occurs in males who engage in activities that expose the hypothenar eminence to repetitive hand injuries. Workers using vibrating hand tools are commonly affected. Sportsmen who use their hands extensively in sports activities such as baseball, handball, karate, and weightlifting or dumbbell training are also affected. Patients usually present with palm pain, paresthesia, and numbness with cold fingers and pallor, usually affecting the dominant hand. HHS can be mistaken for Raynaud’s disease. Raynaud’s disease is defined as episodic ischemia of the fingers and toes, clinically presenting as pallor (arterial vasospasm), cyanosis (deoxygenated static venous blood), and rubor (reactive hyperemia).
Eosinophilic fasciitis (Shulman’s syndrome) is a rare condition with scleroderma-like illness characterized clinically by inflammatory swelling and induration of the arms and legs. Patients with eosinophilic fasciitis are usually females presenting with painful thickening and induration of the skin and subcutaneous tissues of the affected limb. The disease may affect the upper limbs, trunk, and lower limbs but spares the face. Raynaud’s phenomenon is usually not present, and organs are not affected. The skin is typically thickened with orange-peel appearance. Bilateral symmetrical muscle weakness and stiffness of the joint may occur. Pathologically, there is inflammation and infiltration of the superficial muscle fasciae by lymphocytes, plasma cells, and occasionally eosinophils. Laboratory findings show high ESR, blood eosinophilia (characteristic), and hyperglobulinemia. Diagnosis is usually based on MRI and laboratory findings; however, definite diagnosis requires full-thickness skin-to-muscle biopsy.
How can you differentiate between hypothenar hammer syndrome and Raynaud’s disease?
HHS has a male predominance, while Raynaud’s disease has a female predominance.
HHS is an occupational disease, while Raynaud’s disease is a primary disease or secondary to systemic disease.
HHS has an asymmetric distribution (affects one hand), while Raynaud’s disease is typically symmetrical, affecting the hands or toes.
Signs on Radiographs
Resorption of the terminal phalanges (acro-osteolysis) of the hands and the distal portion of the radius and ulna are the most common radiological features of scleroderma (80 %).
Mandibular resorption resembling “Gorham syndrome osteolysis” may be seen.
Soft-tissue calcinosis may be seen, especially in the digits (Figs. 8.1.4 and 8.1.5).

Fig. 8.1.4
Plain thumb radiograph of a patient with scleroderma shows fingertip calcinosis (arrowhead)

Fig. 8.1.5
Lateral plain elbow radiograph of a patient with scleroderma shows calcinosis around the elbow joint (arrowheads)
Widening of the periodontal space on dental radiographs may be seen.
Pulmonary fibrosis can be seen in advanced chronic stages of scleroderma.
Signs on Barium Swallow
The esophagus in CREST syndrome shows weak peristalsis with no stripping waves (Fig. 8.1.6). The esophagus may show fine, wavy horizontal lines due to muscular contraction of the esophagus wall (Feline esophagus).

Fig. 8.1.6
Anteroposterior barium swallow radiograph of the esophagus in a patient with scleroderma shows poor esophageal motility (arrowheads)
Signs on MRI
In linear scleroderma, there are intracranial parenchymal calcifications affecting mainly the thalami, and the basal ganglia ipsilateral to the skin lesion may be seen. Progressive multiple brain aneurysms can be seen in linear scleroderma.
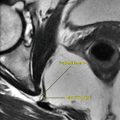
In hypothenar hammer syndrome, the axial wrist images will show hyperintense mass usually seen on T1W images located around the ulnar artery at the level of the hook of the hamate, representing hematoma or thrombus (Fig. 8.1.7).

Fig. 8.1.7
Axial T2W wrist MR illustrations show high signal intensity at the tip of the hook of hamate within the Gyon’s canal representing hematoma of the ulnar artery (arrowhead)
In deep morphea, there is T2 hyperintensity signal observed over the skin and subcutaneous tissue that may involve the muscles and the bone beneath. The bone shows bone marrow edema signal without bone erosions. Contrast enhancement of the affected tissues reflects ongoing inflammatory reaction. Enhancement around the tendons may be observed due to inflammation of the synovial sheath (synovitis).
In eosinophilic fasciitis, there is increased thickening and T2 signal intensity of the superficial muscle fasciae with marked contrast enhancement after contrast injection (Fig. 8.1.8). Characteristically, there is little or no signal change within muscles, and the pathological changes are confined only to the superficial muscle fasciae and to a lesser degree to the deep muscle fasciae.

Fig. 8.1.8
Axial T1W postcontrast, fat-sat, thigh MR illustration demonstrates the typical findings in eosinophilic fasciitis. Notice the marked thickening and enhancement of the superficial and deep fascial planes with no signal intensity or contrast enhancement of the muscles of the subcutaneous tissues
Further Reading
Abudakka M, et al. Hypothenar hammer syndrome: rare or underdiagnosed? Eur J Vasc Endovasc Surg. 2006;32:257–60.
Ahathya RS, et al. Systemic sclerosis. Indian J Dent Res. 2007;18:27–30.
Baumann F, et al. MRI for diagnosis and monitoring of patients with eosinophilic fasciitis. AJR Am J Roentgenol. 2005;184:169–74.
Bologina JL, et al. Lines of Blaschko. J Am Acad Dermatol. 1994;31:157–90.
Christen-Zaech S, et al. Pediatric morphea (localized scleroderma): review of 136 patients. J Am Acad Dermatol. 2008;59:385–96.
Genchellac H, et al. Hypothenar hammer syndrome: gray-scale and color Doppler sonographic appearance. J Clin Ultrasound. 2008;36(2):98–100. doi:10.1002/jcu.
Grosso S, et al. Linear scleroderma associated with progressive brain atrophy. Brain Dev. 2003;25:57–61.
Horger M, et al. MRI findings in deep and generalized morphea (localized scleroderma). AJR Am J Roentgenol. 2008;190:32–9.
Jacobson L, et al. Superficial morphea. J Am Acad Dermatol. 2003;49:323–5.
James WD, et al. Nodular (keloidal) scleroderma. J Am Acad Dermatol. 1984;11:111–4.
Krell JM, et al. Nodular scleroderma. J Am Acad Dermatol. 1995;32:343–5.
Kreitner KF, et al. Hypothenar hammer syndrome caused by recreational sports activities and muscle anomaly in the wrist. Cardiovasc Intervent Radiol. 1996;19:356–9.
Mueller LP, et al. Hypothenar hammer syndrome in sports. Knee Surg Sports Traumatol Arthrosc. 1996;4:167–70.
Robitschek J, et al. Treatment of linear scleroderma “en coup de saber” with AlloDerm tissue matrix. Otolaryngol Head Neck Surg. 2008;138:540–1.
Soma Y, et al. Frontoparietal scleroderma (en coup de saber) following Blaschko’s lines. J Am Acad Dermatol. 1998;38:366–8.
8.2 Lipoid Proteinosis (Urbach–Wiethe Disease)
Lipoid proteinosis (LP) is a rare, autosomal recessive disease characterized by infiltration of the skin, oral cavity, larynx, vocal cords, and internal organs by a hyaline material composed of carbohydrates, proteins, and lipids.
LP is caused by defective basement membrane collagen metabolism. The patient commonly presents with hoarseness of voice since infancy due to deposition of the hyaline material within the vocal cords. Beaded, whitish papules along the margins of the eyelids (Blepharosis moniliformis) are classical features of this disease (Fig. 8.2.1). Pock-like scars over the face and the body, waxy papules, less mobile tongue, and thickened oral mucosa with yellowish tinges are other common findings. Deposition of the hyaline material in the scalp can lead to patchy loss of hair (alopecia areata).

Fig. 8.2.1
Multiple images from a 28-year-old patient with lipoid proteinosis show the dermatological features of this disease. In (a), there are multiple psoriatic-like lesions over the elbow. In (b), a whitish papule (blepharosis moniliformis) along the margin of the upper eyelid can be seen (white arrowhead). In (c), the tongue is thickened and shows multiple nodules (black arrowhead). In (d), there is a focal area with reduced hair on the scalp (arrow). The patient has a history of hoarseness of voice since the age of 3 years
Hyaline deposition can be found in some cases in the trachea, stomach, esophagus, testes, pancreas, and vagina.
Diabetes mellitus, epilepsy, and calcified cerebral vessels can be seen associated with LP occasionally. Diagnosis can be confirmed by pathological skin biopsy. The hyaline material shows positive periodic acid–Schiff (PAS) stain result. Differential diagnoses of LP in adults include amyloidosis, lipoidoses, and myxoedema.
Signs on Chest Radiographs
In severe cases, LP can present as a bilateral alveolar lung disease that mimics lung edema. This pattern is seen due to deposition of the hyaline material within the alveoli.
Signs on CT
Thickening and infiltration of the vocal cords by a hypodense hyaline material can be observed (Figs. 8.2.2 and 8.2.3).

Fig. 8.2.2
Bronchoscopic image (a) correlated with axial CT image (b) of the hypopharynx shows multiple submucosal nodules. After biopsy these lesions, the results stated that these nodules are composed of hyaline lipoid material deposited within the submucosa. The nodules in (b) are almost completely replacing the valleculae (arrowheads)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree