Desmoid
Michael P. Federle, MD, FACR
Kathleen E. Jacobs, BA
Key Facts
Terminology
Aggressive fibromatosis
Imaging
Abdominal desmoids can be solitary or multiple
Tend to invade locally and recur and grow very rapidly, especially in Gardner syndrome
Mesenteric desmoids
± displacement, retraction, compression of bowel loops and mesenteric vessels
± infiltration into adjacent organs and musculature
Abdominal wall desmoids
Involve rectus or oblique muscles (incision sites)
Usually solid with well-defined margins
Top Differential Diagnoses
Leukemia and lymphoma, abdominal signs
Omental or mesenteric metastases
Carcinoid tumor
Pancreatic pseudocyst
Abdominal mesothelioma
Sclerosing mesenteritis
Clinical Issues
Usually associated with Gardner syndrome
18-20% of patients with Gardner syndrome develop desmoids
Most often in women of childbearing age
75% of patients with desmoid tumors have had prior abdominal surgery
Encasement of mesentery and bowel → ischemia and obstruction → progressive resection of bowel → short gut syndrome → small bowel transplantation
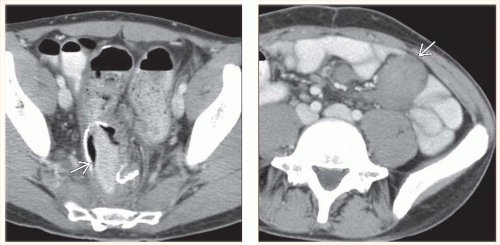 (Left) Axial CECT in a 35-year-old man with Gardner syndrome who had a colectomy at age 30 shows the suture line  for the ileoanal pouch that was anastomosed to the anus. (Right) Axial CECT in the same patient shows a small soft tissue density mesenteric mass for the ileoanal pouch that was anastomosed to the anus. (Right) Axial CECT in the same patient shows a small soft tissue density mesenteric mass  , a typical desmoid in this setting. This caused no symptoms and was not resected. , a typical desmoid in this setting. This caused no symptoms and was not resected. |
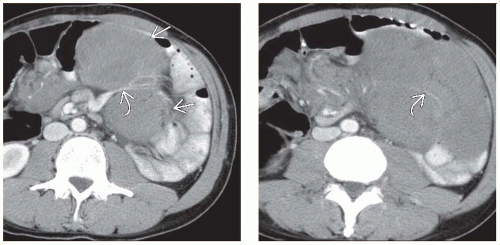 (Left) Axial CECT in the same patient 8 months later shows rapid growth of the mesenteric desmoids  . Note the encasement of the mesenteric vessels . Note the encasement of the mesenteric vessels  . (Right) Axial CECT in the same patient shows the mesenteric desmoid encasing mesenteric vessels . (Right) Axial CECT in the same patient shows the mesenteric desmoid encasing mesenteric vessels  and the bowel. The patient was treated with complete resection of the small bowel and mesentery followed by small bowel transplantation. and the bowel. The patient was treated with complete resection of the small bowel and mesentery followed by small bowel transplantation. |
TERMINOLOGY
Synonyms
Aggressive fibromatosis
Definitions
Rare, benign, locally aggressive, nonencapsulated tumor of connective or fibrous tissue
IMAGING
General Features
Best diagnostic clue
Small bowel mesentery or abdominal wall mass arising from scar of prior surgery
Location
Abdominal
Mesentery: Small bowel (most common)
Musculature: Rectus, internal/external oblique, psoas, pelvic (rare)
Retroperitoneum
Extraabdominal
Bladder, ribs, and pelvic bones
Size
Mass may range from 4-20 cm
Morphology
Well- or ill-defined, tan or white, hard fibrous mass
Clear, lobulated margin (75%); ill-defined, infiltrative (25%)
Key concepts
Abdominal desmoids can be solitary or multiple
Locally aggressive mesenteric primary tumor
Tend to arise in musculoaponeurotic planes
Tend to invade locally and recur and grow very rapidly, especially in Gardner syndrome
May involve bowel loops, bladder, ribs, pelvic bones
Sometimes classified as low-grade fibrosarcoma or subgroup of fibromatosis
Usually associated with Gardner syndrome
Familial polyposis coli, osteomas, dental defects, congenital pigmented lesions of retina
Epidermoid (sebaceous) cyst and fibromas of skin
Periampullary, adrenal, thyroid, and liver carcinomas
75% of patients with desmoid tumors have had prior abdominal surgery
18-20% of patients with Gardner syndrome develop desmoids
Accounts for 45% of fibrous lesions in Gardner
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


