Childhood aneurysms have special characteristics different from adults’ aneurysms. Their features were found to significantly differ from aneurysms in adults especially in their gender prevalence, location, morphology and underlying etiology. Treatment options include both surgical and endovascular methods. Whenever possible, endovascular treatment for pediatric aneurysms is the recommended approach, since it offers both reconstructive and deconstructive techniques, durable results and better clinical outcome.
Although rare, intracranial aneurysms in children have been discussed thoroughly in the literature . Their features have been found to differ significantly from aneurysms in adults, especially in their gender prevalence, location, morphology, and underlying etiology . During the neonatal and infantile period the differences from adult aneurysms are striking, whereas during adolescence the adult aneurysm characteristics become progressively more apparent . The versatility of these aneurysms represents a unique management challenge.
Incidence and gender prevalence
Intracranial aneurysms in the pediatric age group represent less than 5% (0.6%–4.6%) of the total number of intracranial aneurysms in the general population . In children, boys are more likely to harbour aneurysms than are girls . After puberty, this ratio changes to the point that, in adults, women have between three to five times more aneurysms then men . In reports that include relatively older children, the male dominance has been less evident , with almost a 1:1 ratio between males and females. Others have found a female dominance under the age of 2 years .
Clinical presentation
Children with intracranial aneurysms present with subarachnoid hemorrhage about 70% of the time . The incidence of hemorrhage is reported to be as high as 82% if only infants and children below 5 years of age are considered . Subarachnoid hemorrhage presentation appears to decrease progressively with age and is as low as 45% if only children over 5 years of age are considered . Pediatric patients with giant aneurysms present with subarachnoid hemorrhage 35% of the time . Symptoms related to mass effect occur in 20% of all children as the presenting symptom of an intracranial aneurysm . Again, this percentage varies among the different age groups and is reported to be as high as 45% in the 5- to 18-year age group . Other clinical presentations such as seizures and stroke are uncommon and occur in less than 10% of cases .
In the authors’ recent series , a relatively low percentage of patients presented with subarachnoid hemorrhage when compared with previous series . Children presented most commonly with a neurologic deficit with or without infarct (45%). This presentation was followed by headaches (33%). Subarachnoid hemorrhage or intracerebral hematoma was encountered in 27% of patients. Focal neurologic symptoms including those from mass effect were the most common presentation in some other studies , especially those including older children (5 to 18 years of age) , such as in the authors’ patient group.
Clinical presentation
Children with intracranial aneurysms present with subarachnoid hemorrhage about 70% of the time . The incidence of hemorrhage is reported to be as high as 82% if only infants and children below 5 years of age are considered . Subarachnoid hemorrhage presentation appears to decrease progressively with age and is as low as 45% if only children over 5 years of age are considered . Pediatric patients with giant aneurysms present with subarachnoid hemorrhage 35% of the time . Symptoms related to mass effect occur in 20% of all children as the presenting symptom of an intracranial aneurysm . Again, this percentage varies among the different age groups and is reported to be as high as 45% in the 5- to 18-year age group . Other clinical presentations such as seizures and stroke are uncommon and occur in less than 10% of cases .
In the authors’ recent series , a relatively low percentage of patients presented with subarachnoid hemorrhage when compared with previous series . Children presented most commonly with a neurologic deficit with or without infarct (45%). This presentation was followed by headaches (33%). Subarachnoid hemorrhage or intracerebral hematoma was encountered in 27% of patients. Focal neurologic symptoms including those from mass effect were the most common presentation in some other studies , especially those including older children (5 to 18 years of age) , such as in the authors’ patient group.
Etiology of aneurysms in children
In children, as in adults, the etiology of aneurysms is mostly unknown. A clear underlying cause for a childhood aneurysm is found in less than 50% of cases . Although they are often regarded as congenital , as far as being present at birth, neither adult nor pediatric aneurysms are truly congenital in nature . This observation is supported by a large autopsy series that did not detect any incidental aneurysms in children . Thus, the term congenital aneurysm to describe aneurysms in children should probably be abandoned, and the identification of an aneurysm in a child should rather raise the suspicion of an underlying disease affecting the blood vessel wall. A review of published histopathology reports of intracranial aneurysms led to the conclusion that a combination of intraluminal, mural, and extravascular factors are likely responsible for the development of saccular aneurysms . Lasjaunias and colleagues suggested that aneurysms in children must be the expression of various vessel wall dysfunctions producing transient or permanent failure to repair a partial insult. These included, on one hand, “recognized” mutations and “direct” primary triggers (eg, humoral, immune, infectious, trauma) and, on the other hand, “silent” genetic diseases (eg, polycystic kidney disease, fibromuscular dysplasia, Ehlers-Danlos syndrome).
There appears to be a clear association between various disease processes that are known to weaken the matrix of the blood vessel wall and the presence of aneurysms in the pediatric age group, and these intramural factors probably have an important role in the etiology of aneurysms in children . The concept of “segmental identity and vulnerability” is particularly well illustrated in the aneurysmal vasculopathies in children.
Aneurysms in children are traditionally referred to according to their underlying etiology (eg, traumatic, infectious). Because a clear underlying cause for a childhood aneurysm is found in less then 50% of cases , with the lack of a known underlying condition, the remaining aneurysms are named according to their appearance on angiography. Aneurysms are called “berry” or “saccular” when they have a saccular appearance and “dissecting” when the aneurysm has a fusiform appearance and has pre- or postaneurysmal narrowing . The incidence of each type of aneurysm must be adjusted to the patient’s age at presentation. Dissections are dominant during the first 5 years of life, whereas saccular aneurysms are more common in children older than 6 years.
Traumatic aneurysms
Traumatic aneurysms account for about 5% to 39% of pediatric aneurysms . Of these, about 40% involve the distal anterior cerebral artery complex (adjacent to the falx), 35% involve the major vessels along the skull base, and 25% are cortical in location . These children usually present with a hemorrhagic episode 3 to 4 weeks after injury, but immediate bleeding has also been reported . Seventy two percent of children have sustained a closed head injury, 16% a penetrating injury, and the remainder a history of various types of injuries, including surgery . Most post-traumatic aneurysms increase in size on angiographic follow-up before treatment . This finding is secondary to a false or pseudoaneurysm that corresponds to an extravascular space, usually within a hematoma surrounding the aneurysm. Although the evolution of these lesions can sometimes be favorable with spontaneous healing of the leakage point, a mortality rate of 31% has been reported .
Infectious aneurysms
Infectious aneurysms account for 5% to 15% of pediatric aneurysms . The term mycotic arterial aneurysm was proposed by Osler in 1901 to describe aneurysms seen during bacterial endocarditis. This designation has been kept to identify aneurysms associated with an infectious state . Today, the term infectious arterial aneurysm seems more appropriate . Infectious arterial aneurysms may involve the artery directly by continuity from sphenoid sinus or mastoid air cell infections with osteomyelitis and sinus thrombophlebitis or reach the artery via infectious emboli . A direct involvement of the arterial wall is the mechanism most often advocated, with an infectious process progressing from the lumen to the extravascular space . Although these aneurysms can be caused by fungal infections, they are most often of bacterial origin . The most common organism is staphylococcus, followed by streptococcus and other gram-negative organisms . Infectious arterial aneurysms often complicate bacterial endocarditis in infants with congenital or rheumatic heart disease. The time interval between the infectious embolus and the development of an infectious arterial aneurysm including rupture can be as short as 24 to 48 hours. Twenty percent of children with aneurysms of infectious origin die despite antibiotic treatment ( Fig. 1 ) .
Infectious arterial aneurysms associated with HIV
Several reports of aneurysms in children associated with HIV are found in the literature . In children, neurovascular manifestations of AIDS differ markedly from those in adults. Whereas vascular complications in adults usually consist of vascular occlusions associated with distal emboli and complications of thrombocytopenia, in children, cerebrovascular lesions are mostly due to arteritis including arterial sclerosis, vascular occlusions, and the formation of intracranial aneurysms . A few cases of HIV-infected children with multiple fusiform aneurysms have been described . These aneurysms were almost all multifocal fusiform arterial dilatations involving the major vessels of the circle of Willis, predominantly involving the supraclinoid internal carotid artery as well as the basilar artery, not affecting the distal parts of the cerebral arteries. The distal arterial segments showed mostly a typical appearance of arteritis including stenosis and thrombosis .
The pathogenesis of fusiform aneurysms in HIV-infected children has been discussed by several investigators and remains controversial. Some have proposed the vasculopathy to be secondary to an infectious cause . However, it seems that primary arterial wall infection is unlikely, because histologic and bacteriologic analyses of these lesions failed to detect the presence of any infectious agent, and none of the patients had a laboratory confirmed central nervous system infection at the time of the diagnosis. Shah and colleagues suggested that the aneurysms (as well as the arterial thromboses and stenoses) seen in this population with severe immune deficiencies were in fact inflammatory panarteritic lesions involving the vasa vasorum and adventitia, causing ischemia of the arterial wall leading to the destruction of the lamina elastica.
Although childhood HIV lesions were initially considered as relatively specific , similar features have been observed in chronic mucocutaneous candidiasis (CMCC) . CMCC is a rare familial primary immunodeficiency of unknown etiology characterized by recurrent infections of the mucous membranes, nails, and skin with Candida albicans . The association of CMCC with cerebral vasculitis or aneurysm is rare, but the similarities between cerebral aneurysms in CMCC and AIDS are remarkable. CMCC aneurysms are fusiform and present in the same topographic distribution involving the vessels of the base and sparing of the distal territories. This observation supports the concept of “segmental susceptibility” of the cerebral arterial system . It is possible that intracranial aneurysms occurring in children who have CMCC or AIDS reveal areas of the cerebral vasculature that apparently share the same “identity” or vulnerability . The immune disease exposes these areas to specific or nonspecific triggers depending on the pre-existence of a segmental structural weakness.
Aneurysms associated with vascular conditions
A variety of case reports have described the association of aneurysms in the pediatric population with systemic disorders such as collagen vascular diseases. Ehlers-Danlos syndrome, Klippel-Trenaunay syndrome, hereditary hemorrhagic telangiectasia, tuberous sclerosis, moyamoya syndrome, coarctation of the aorta, and fibromuscular hyperplasia have all been documented to occur in association with aneurysms in children . These disease processes that are known to weaken the matrix of the blood vessel wall are clearly associated with the presence of aneurysms in the pediatric age group.
Saccular aneurysms
Most of the aneurysms in the pediatric population (between 46% and 70%) are reported to be of this type . The etiology of saccular aneurysms remains as controversial in the pediatric age group as in adults. Despite their location at the bifurcation point of various vessels, intrinsic hemodynamic factors almost certainly have less of a role in children as compared with in adults. Mural or systemic factors are considered to be more important .
Dissecting aneurysms (nontraumatic)
The frequency of dissecting aneurysms in the pediatric age group is four times that in adults . This type of aneurysm tends to be located at the posterior circulation, especially the P1 and P2 segments of the posterior cerebral artery, supraclinoid internal carotid artery, and middle cerebral artery . In the authors’ experience, most dissecting aneurysms have involved the posterior circulation , which was also true in more than 50% of Lasjaunias’ recent series . Both of these recent series contained a larger number of nontraumatic dissecting aneurysms (18.9% in the authors’ series, 45% in Lasjaunias’ series) when compared with the numbers reported previously in the literature .
The focal arterial stenotic segments that are often observed proximal or distal to a dissecting aneurysm suggest mural damage. Stenotic vessel wall can induce spontaneous thrombosis, and some of the dissecting aneurysms in children heal spontaneously, leading to occlusion of the parent artery . This occlusion is often well tolerated in the child owing to good collateral circulation via the circle of Willis or pial collateral anastomoses. In the Lasjaunias’ series, the time frame for spontaneous thrombosis of dissecting aneurysms was 3 weeks to 7 months .
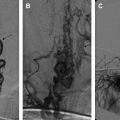
Two types of dissections can be encountered . The first type involves extensive vessel wall damage (fusiform or wide neck “saccular” aneurysms) without evidence of mural hematoma. These aneurysms may present with a deep-seated stroke or a subarachnoid hemorrhage. Early recurrence of rupture often occurs during the first few days, and aggressive treatment is recommended. In the second type, focal lesions can be of large size (giant or large “saccular” aneurysms) with evidence of recent mural hematoma on CT or MR imaging but with no subarachnoid hemorrhage. Presentation is often ischemic, and spontaneous healing with completion of the lumen thrombosis is frequently observed. Medical treatment with aspirin or even anticoagulation is recommended; anti-inflammatory treatment may have to be discussed ( Fig. 2 ) .
Giant aneurysms
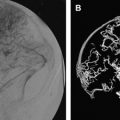
Giant aneurysms are known to be of increased incidence in children, being about four times more common than in adults . Their reported incidence in this age group is between 20% and 45% . Giant aneurysms should not only be distinguished because of their size but also as a group within the dissection category. Repeated small intramural hematomas may lead to formation of the onionskin pattern of thrombotic layers on CT and MR imaging. Children who have giant size aneurysms often present with mass effect and only 35% of the time with subarachnoid hemorrhage . The natural history of these unruptured aneurysms varies depending on their size ( Fig. 3 ) .
Related posts:
 Diagnosis and Endovascular Treatment of Pediatric Spinal Arteriovenous Shunts
Diagnosis and Endovascular Treatment of Pediatric Spinal Arteriovenous Shunts
 Pediatric Neuroanesthesia
Cerebral Sinovenous Thrombosis in Children
Pediatric Neuroanesthesia
Cerebral Sinovenous Thrombosis in Children
 Overt and Incomplete (Silent) Cerebral Infarction in Sickle Cell Anemia: Diagnosis and Management
Overt and Incomplete (Silent) Cerebral Infarction in Sickle Cell Anemia: Diagnosis and Management
 Vein of Galen Aneurysmal Malformations
Current Endovascular Management of Maxillofacial Vascular Malformations
Vein of Galen Aneurysmal Malformations
Current Endovascular Management of Maxillofacial Vascular Malformations
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


