12-year-old female with discharge from right buttock
1. What are the findings?
2. What are the complications of this entity?
3. What is the most likely microorganism that may complicate this entity?
4. What is the differential diagnosis?
5. What are the treatment options?
Foreign body in right buttock 273
Case ranking/difficulty: | Category: Pelvis |
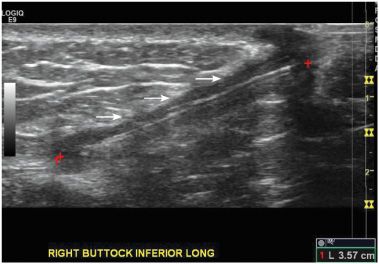
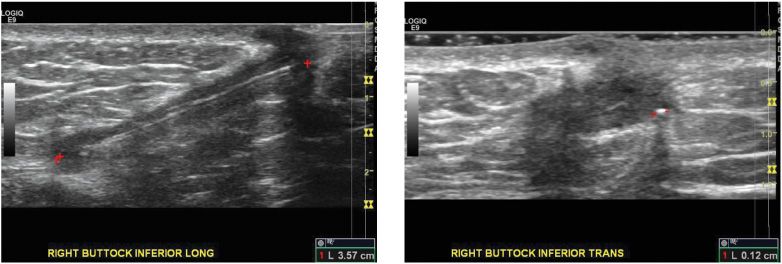
Longitudinal sonogram of the right inferior buttock reveals that a linear, long, thin foreign body (arrows) enters deep the buttock. The tip is seen at 1.6 cm depth. Edema surrounds the foreign body.
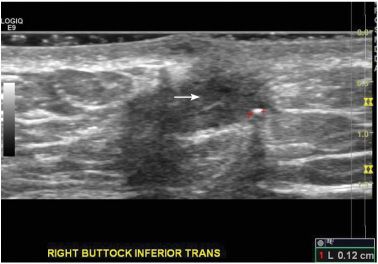
Transverse sonogram of the right inferior buttock reveals a foreign body entering deep into the buttock (arrow). Edema surrounds the foreign body.
Answers
1. In the right inferior buttock, there is a linear, thin foreign body surrounded by edema.
2. Complications may include infection, inflammation, and abscess formation.
3. The most likely microorganism that may complicate the case and cause infection is Staphylococcus aureus.
4. The entity shown is an obvious foreign body in the subcutaneous tissue of the buttock and no differential diagnosis is included.
5. The treatment options are antibiotics and tetanus prophylaxis. Surgical removal should be performed.
Suggested Reading
Ludin M. Foreign body in buttock. Radiol Clin. 1951;20(3):185-186.
7-year-old male with swelling of the right foot

1. What are the findings?
2. What are the complications of this entity?
3. What is the least sensitive modality for detection of foreign body in the foot?
4. What is the most common microorganism that causes infection in this case?
5. What are the treatment options?
Foreign body in the foot 219
Case ranking/difficulty: | Category: Lower extremities |

Frontal view of the right foot reveals a radio-opaque foreign body seen in the soft tissue medial to the right calcaneum (arrow). The foreign body was a broken toothpick.

Lateral view of the right foot reveals a radio-opaque foreign body seen in the plantar soft tissue beneath the right calcaneum (arrow). The foreign body was a broken toothpick.
Answers
1. Foreign body is seen in the soft tissue of the foot below the calcaneum.
2. Complications may include inflammation, infection, abscess formation around the foreign body, and scarring.
3. MRI (58%) and CT (63%) scan have higher sensitivity to detect foreign body than the radiographs (29%).
4. The most common microorganism that can complicate and causes infection of foreign body in soft tissue is Staphylococcus aureus.
5. Treatment options include removal of foreign body, tetanus prophylaxis, and antibiotics if infection is present.
Suggested Readings
Gregori D, Foltran F, Passali D. Foreign body injuries in children: need for a step forward against an old yet neglected epidemic. Paediatr Perinat Epidemiol. 2011;25(2):98-99.
Pattamapaspong N, Srisuwan T, Sivasomboon C, et al. Accuracy of radiography, computed tomography and magnetic resonance imaging in diagnosing foreign bodies in the foot. Radiol Med. 2013;118(2):303-310.
Pogoreli Z, Bioi M, Bekavac J. An unusual foreign body in the foot: traumatic implantation of a human tooth. J Foot Ankle Surg. 2011;50(2):225-226.
1-day-old Male

1. What is the pattern of the deformity seen in the thoracolumbar spine?
2. What is the most common spinal anomaly that causes such a case?
3. What is the incidence of spinal cord abnormalities associated with congenital scoliosis?
4. What are the associated anomalies?
5. What are the treatment options?
Congenital scoliosis 631
Case ranking/difficulty: | Category: Spine |

Frontal view of the thoracolumbar spine demonstrates severe scoliosis. The arrows demonstrate right-sided convexities, and the arrowhead demonstrates left-sided convexity.
Answers
1. Scoliosis is noted. There is right-sided convexity centered on the mid thoracic spine. Left-sided convexity is noted centered on T11. There is right-sided convexity centered on the mid lumbar spine. Lateral wedging of the vertebral body T11 is seen.
2. Hemivertebra is the most common anomaly that causes congenital scoliosis by acting as an enlarging wedge on the affected side of the spine. The degree of scoliosis produced by hemivertebra depends on their type/site/number/relationship to each other and the patient’s age.
3. The incidence of spinal cord abnormalities associated with congenital scoliosis is reported to range from 20% to over 50% in most of the series.
4. The most common of anomaly sites are genitourinary tract, cardiac system, the spinal cord, and the cervical spine. Many are part of VACTREL association, and also incidence of Klippel–Feil syndrome is high.
5. Braces, orthopedic spinal fusion and, in some cases, hemiarthrodesis are treatment options.
Suggested Readings
Jog S, Patole S, Whitehall J. Congenital scoliosis in a neonate: can a neonatologist ignore it? Postgrad Med J. 2002;78:469-472.
McMaster MJ, David CV. Hemivertebra as a cause of scoliosis. A study of 104 patients. J Bone Joint Surg Br. 1986;68:588-595.
Oestreich AE, Young LW, Poussaint TY. Scoliosis circa 2000: radiologic imaging perspective 1. Diagnosis and pretreatment evaluation. Skeletal Radiol. 1998;27:591-605.
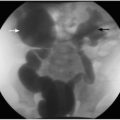
13-year-old male with developmental delay and scoliosis

1. What are the findings?
2. What is the Hilgenreiner line?
3. What is the Perkin’s line?
4. What is the normal acetabular angle?
5. In which quadrant formed by the intersection of the Hilgenreiner and Perkin’s lines should the normal femoral head project?
Congenital dislocation of the hips 402
Case ranking/difficulty: | Category: Pelvis |

Pelvis x-ray in a frontal view reveals superior dislocation of both femoral heads. Both acetabula are shallow (arrowheads); pseudoacetabulum has been formed bilaterally (arrows) secondary to molding of the displaced femoral heads with the iliac bones.

Pelvis radiograph in abduction view reveals superior dislocation of both femoral heads. Both acetabula are shallow (arrowheads); pseudoacetabulum has been formed bilaterally (arrows) secondary to molding of the displaced femoral heads with the iliac bones.

Frontal radiograph of the thoracolumbar spine reveals scoliosis. There is curvature with right-sided convexity. The scoliosis is centered on T6 (arrow).
Answers
1. There is bilateral dislocation of the femoral heads superiorly with formation of bilateral pseudoacetabulum. Scoliosis is seen. The patient has tracheostomy tube.
2. Hilgenreiner line is a horizontal line between the two triradiate cartilages.
3. The Perkin’s line is drawn at the outer acetabular margin and is perpendicular to the Hilgenreiner line.
4. The normal acetabular angle measures slightly less than 30 degrees.
5. Both femoral heads should project in the inner lower quadrants formed by the intersection of the Hilgenreiner and Perkin’s lines.
Suggested Readings
Kirks DR, Griscom NT. Practical Pediatric Imaging Diagnostic Radiology of Infants and Children. Philadelphia, PA: Lippincott-Raven; 1998.
Ozonoff MB. Pediatric Orthopedic Radiology. 2nd ed. Philadelphia, PA: WB Saunders; 1992.
2 years and 4 months old male with bowing of the lower extremities
1. What is the diagnosis?
2. What are the imaging findings?
3. What is the possible etiology of this entity?
4. What is the normal metaphyseal-diaphyseal angle in an infant less than 2 years?
5. What should be the main differential diagnosis of this entity in a toddler less than 2 years?
Blount’s disease 345
Case ranking/difficulty: | Category: Lower extremities |

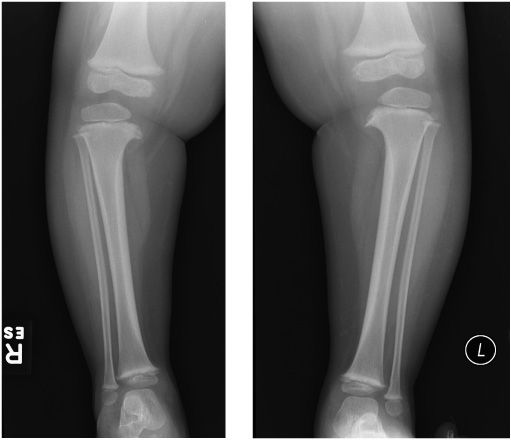
Frontal radiograph of the right leg reveals medial beaking of the proximal wtibial metaphysis (arrow) Tibia vara noted.

Frontal radiograph of the left leg reveals medial beaking of the proximal tibial metaphysis (arrow) Tibia vara noted.
Answers
1. The diagnosis is Blount’s disease or tibia vara.
2. Imaging findings include varus deformity of the lower extremities (tibia vara), medial beaking, and fragmentation of the proximal tibial metaphysis.
3. Blount’s disease is a developmental disease caused by excessive forces on the proximal metaphyses of the tibia in toddlers when they start to walk. During the growth period, altered endochondral bone formation may be a contributing factor for the development of this entity.
4. The normal metaphyseal-diaphyseal angle in an infant less than 2 years is less than 11 degrees.
5. The main differential diagnosis of Blount’s disease in a toddler less than 2 years is physiologic bowing of the lower extremities.
Suggested Readings
Hofmann A, Jones RE, Herring JA. Blount’s disease after skeletal maturity. J Bone Joint Surg Am. 1982;64(7):1004-1009.
Iwasawa T, Inaba Y, Nishimura G, Aida N, Kameshita K, Matsubara S. MR findings of bowlegs in toddlers. Pediatr Radiol. 1999;29(11):826-834.
Sabharwal S. Blount’s disease. J Bone Joint Surg Am. 2009;91(7):1758-1776.
11-year-old male with bony lump in the knee

1. What is the diagnosis?
2. What are the complications of this case?
3. What are the findings?
4. What is the sign of malignant degeneration in MRI?
5. What is the percentage risk for malignant degeneration?
Hereditary multiple osteochondromatosis 368
Case ranking/difficulty: | Category: Generalized diseases |

The left knee demonstrates multiple bony excrescences arising from the metaphyses of the bones. These excrescences have extension of the periosteum and form an obtuse angle with the bone (arrows).

The right knee demonstrates multiple bony excrescences arising from the metaphyses of the bones. These excrescences have extension of the periosteum and form an obtuse angle with the bone (arrows).

The right wrist demonstrates multiple bony excrescences arising from the metaphyses of the bones. These excrescences have extension of the periosteum and form an obtuse angle with the bone (arrows).

The left wrist demonstrates multiple bony excrescences arising from the metaphyses of the bones. These excrescences have extension of the periosteum and form an obtuse angle with the bone (arrows).
Answers
1. The diagnosis is hereditary multiple osteochondromatosis or hereditary multiple exostosis.
2. Tendons, nerves, or blood vessels may be trapped around osteochondromas, leading to symptoms. Symmetric or asymmetric impaired body growth is seen. Malignant degeneration can occur in about 1 to 20% of the cases.
3. There are bone excrescences arising from the metaphyses of long bones. The periosteum is in continuation with the excrescence. The pattern of these excrescences in hereditary multiple exostosis is being sessile. In most patients with single exostosis, the excrescence is pedunculated.
4. The MRI sign of malignant degeneration is cartilage cap thickness of more than 1 cm.
5. The risk for malignant degeneration is 1 to 20%.
Suggested Readings
Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, Bai M. Osteochondromas: review of the clinical, radiological and pathological features. In Vivo. 2008;22(5):633-646.
Reijnders CM, Waaijer CJ, Hamilton A, et al. No haploinsufficiency but loss of heterozygosity for EXT in multiple osteochondromas. Am J Pathol. 2010;177(4):1946-1957.
15-year-old male with right knee pain and limping

1. What is the diagnosis?
2. What is the most common location of this entity?
3. What is the second most common location of the entity shown?
4. What are the symptoms of focal chondral lesion?
5. What are the treatment options?
Osteochondral defect 216
Case ranking/difficulty: | Category: Lower extremities |

Frontal radiograph of the knees reveals a lucent defect in the lateral condyle of the right knee (arrow).

Lateral radiograph of the right knee reveals a lucent defect in the lateral condyle (arrow).

Coronal MRI T2 of the right knee reveals a low signal seen in the lateral condyle (arrow).
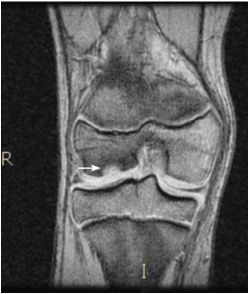
Coronal MRI, MPGR of the right knee reveals a high signal in the lateral condyle, representing cartilage (arrow).
Answers
1. The diagnosis is osteochondral defect.
2. The most common location is femoral condyle.
3. The second most common location is the dome of the talus.
4. Symptomatic focal chondral lesions present as pain, swelling, locking, and athletic dysfunction.
5. Treatment options are arthroscopic surgery, conservative therapy, autologous chondrocyte implantation, allografts implantation, and microfracture surgical technique.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


