Elbow Trauma
The surgical treatment of adult elbow trauma, including traumatic elbow instability, has evolved rapidly in recent years because problems have been better defined and useful concepts and techniques have been established.1 The lateral rather than the medial collateral ligament is now the focus of elbow stability, along with the coronoid process. Most simple elbow dislocations2 and isolated partial radial head fractures2–4 recover well without surgery, but the majority of other injuries to the proximal radius and ulna benefit from surgery. Each specific complex injury type is not very common. When facing complex elbow injuries, surgeons must rely on a familiarity with normal and pathological anatomy of the elbow and a variety of repair techniques in order to obtain the best outcome possible.
Anatomy
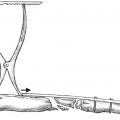
The olecranon and coronoid processes of the proximal ulna form the trochlear notch that articulates with the trochlea of the humerus. The trochlear notch has olecranon and coronoid articular facets separated by the relatively nonarticular transverse groove of the trochlear notch (Fig. 17.1). The trochlear notch prevents anterior-posterior translation of the ulna on the humerus and also provides varus, valgus, and rotational stability to the elbow. Because of its bony architecture, elbow stability is greatest in flexion and decreases with extension. The stability provided by the ulnohumeral articulation gradually decreases as the proximal ulna is incrementally resected.5 The triceps inserts on the dorsal surface of the olecranon, blending with the periosteum and the forearm fascia.

The coronoid process is the anterior extension of the trochlear notch. It serves as the point of insertion of the anterior capsule and the anterior band of the medial collateral ligament (MCL), which inserts on the sublime tubercle of the anteromedial base of the coronoid process (Fig. 17.1).6 The brachialis muscle extends slightly distal to the coronoid on the anterior surface of the ulna. The MCL is made up of anterior, posterior, and transverse bands. The anterior band is the most discrete structure and the most important for valgus elbow stability.7 It originates from the midportion of the undersurface of the medial epicondyle and also inserts on the sublime tubercle of the coronoid process. The lateral aspect of the coronoid is continuous with the radial (lesser sigmoid) notch of the ulna.
The radial head articular surface is concave and articulates with the convex capitellum of the distal humerus. There is an angulation (~ 15 degrees) of the radial neck with respect to the radial shaft. Approximately 240 degrees of the outside circumference of the radial head articulates with the lesser sigmoid notch of the proximal ulna and is covered by hyaline cartilage.8,9 The remaining anterolateral third is not covered by articular cartilage and is also the area most often fractured. The proximal radioulnar joint is stabilized by the annular and quadrate ligaments and the interosseous membrane.10
The lateral collateral ligament complex is the most important stabilizer of the elbow.1 Its effect is most apparent when testing posterolateral rotatory (rather than varus) stability. Although some authors have emphasized the importance of the lateral ulnar collateral ligament itself,11 others have found posterolateral rotatory stability to be more complex, with contributions from the annular ligament and the fascia of the common extensor musculature.12
Handling of the skin around the elbow is straightforward because there is an extensive longitudinal collateral blood supply. A direct posterior skin incision provides access to nearly the entire elbow with the elevation of broad, full-thickness skin flaps.13 It also limits the potential for injury to cutaneous nerves because they are kept in the flaps.14 More limited lateral or medial incisions and simultaneous separate medial and lateral exposures can also be used, depending on the particular injury.
Radial Head Fractures
The management of fractures of the radial head varies substantially depending on whether the fracture is an isolated injury or part of a more complex injury with compromised stability of the elbow or forearm.15 With isolated, nondisplaced, or minimally displaced radial head fractures, the goal is to restore or maintain forearm rotation, which is nearly always possible with nonoperative treatment.3,16–19 In complex injuries, repair or replacement of the radial head is desirable in order to maintain its contribution to elbow and forearm stability.1,20–22
Open reduction and internal fixation of comminuted radial head fractures is much less predictable than operative repair of simple fractures.15,23 The risk of early fixation failure, eventual nonunion and collapse of the fracture, and restriction of forearm rotation15 have made a metal prosthesis more appealing in the treatment of radial head fractures associated with destabilizing injuries of the forearm and elbow.24
Classification
Mason′s18 classification of radial head fractures is popular but often misrepresented. He classified radial head fractures into three types: nondisplaced (type 1), displaced partial articular (type 2), and displaced and comminuted fractures involving the entire head (type 3). Johnston25 suggested a fourth category for radial head fractures associated with elbow dislocations; however, this category is not useful for two reasons: (1) there are several injury patterns that have an associated fracture of the radial head, all of which merit clear distinction from simple isolated fractures; and (2) regardless of the overall injury pattern, the specific characteristics of the fracture are important in determining management and prognosis. Mason did not account for fractures of the radial neck (those with the articular surface intact) in his classification system.
Mason′s classification is often reported along with criteria for acceptable size and displacement of the fragments as measured on radiographs. These radiographic criteria are not validated, and such measurements are likely to be unreliable based on variations in patient positioning for radiographs and the measurement techniques used.
There are additional injury factors that affect the management and prognosis of radial head fractures but are not consistently accounted for in classification systems. For both partial and complete articular fractures (Mason types 2 and 3), the number and size of fracture fragments is important. In many cases there are fragments that are too small for internal fixation or are lost in the soft tissues. It is also common to find fragments with little or no subchondral bone, particularly in older individuals. These fragments are difficult or impossible to repair. There is often articular impaction (Fig. 17.2). When central articular fragments are impacted, realignment leaves them with little support, and bone grafting may be needed in addition to internal fixation. Major portions of the radial head may be impacted; this is often not apparent until it is noted that the smaller fragments cannot be repositioned accurately. Finally, there may be central impaction with expansion of the radial head outward, which may be unsalvageable. All of these factors can be difficult to recognize and define. When the specific criterion of the number of fracture fragments is used, greater than three articular fragments (as suggested by Muller et al′s26 comprehensive classification of fractures) has been associated with greater problems after operative fixation.15

It is important to distinguish fractures of the radial head associated with injury to the interosseous ligament of the forearm—the so-called Essex-Lopresti lesion.27 Such injuries are challenging to treat when recognized acutely but are associated with very poor and practically unsalvageable results when the forearm ligament injuries are initially overlooked.28
Finally, radial head fractures are an inherent part of posterior Monteggia fractures and posterior olecranon fracture-dislocations, present in over two thirds of patients with these injury patterns.29–32
Nonoperative Treatment
Partial fractures of the radial head articular surface (Mason type 2) that are not associated with other fractures or ligament injuries usually do very well with nonoperative treatment in our experience, although at least one study has questioned this assertion.33 To our knowledge, there are no data to support the use of radiographic measurements (e.g., greater than 2 mm of articular surface incongruity, fragment involving greater than 30% of the joint) in deciding on operative or nonoperative treatment. Because radiocapitellar arthritis is not a common sequela of this injury, the most important issue is whether the fracture limits forearm rotation by compromising the proximal radioulnar joint. Initially, patients may be in too much pain to demonstrate forearm rotation; however, reexamination in a few weeks or aspiration and infiltration of the elbow joint with local anesthetic can help determine if there is a bony block to rotation. Nonoperative treatment can be considered if forearm motion is not restricted.
Comminuted fractures of the entire radial head nearly always occur as part of a complex injury to the forearm or elbow.34 The treatment of Mason type 3 fractures of the radial head should be predicated on the high likelihood of associated ligament injury or fracture. For this reason, non-operative treatment (or simple excision) of type 3 fractures should be considered with great caution. Type 3 fractures also have a high likelihood of restricting forearm rotation if treated nonoperatively.
The major risk when treating isolated fractures of the radial head that do not restrict forearm rotation is elbow stiffness. Although it is reasonable to apply a sling or splint to the elbow for comfort immediately after the injury, patients should realize that their recovery from the injury is directly dependent on confident active use and motion exercises of the elbow as soon as possible after the injury.18,19 Immobilization or failure to exercise the elbow within the first 2 weeks can cause permanent elbow stiffness. There should be little concern regarding fracture displacement or nonunion because nonunion of nonoperatively treated radial head fractures is uncommon and usually asymptomatic and inconsequential.35–37
Surgical Treatment
Indications
Excision of the radial head without replacement is a reasonable consideration in any patient who does not have either an Essex-Lopresti injury or a terrible triad fracture of the elbow (a dislocation with fractures of the radial head and coronoid), but it should be used with great caution. When the stability of the forearm and elbow can be ensured, repair or replacement of the radial head has the relative advantages of supporting the elbow for vigorous activities such as throwing and heavy work and perhaps protecting the ulnohumeral joint from early arthrosis.38 When the elbow is stable, excision of the radial head without prosthetic replacement is still a very useful treatment option in older patients with limited functional demands, and select younger patients. After excising the radial head, the elbow and forearm must be carefully tested for instability using the push-pull test to be certain that the interosseous ligament of the forearm is intact and testing to see if the elbow dislocates in extension under the force of gravity.39
Because the long-term performance of radial head prostheses is uncertain, it is preferable to repair the radial head when possible. Most partial (Mason type 2) fractures of the radial head are amenable to operative fixation. However, partial head fractures that consist of multiple small fragments may be difficult to repair. These complex partial radial head fractures should be considered for prosthetic replacement in the setting of troublesome injury patterns such as the Essex-Lopresti or the terrible triad. Early failure of fixation in these injuries could compromise elbow or forearm stability and lead to substantial problems.
Surviving the Night
Radial head fractures are rarely emergencies. Complex elbow or forearm injuries, proximal forearm gunshot wounds,40 and combined unstable wrist and elbow injuries in particular are at risk for forearm compartment syndrome.41 The key with radial head fractures is recognizing longitudinal forearm instability, and ensuring stability of the forearm and elbow, but these can be planned and accomplished during the first week or so.
The results of the operative repair of fractures involving the entire radial head (Mason type 3) are much less predictable. When there are more than three fragments, missing fragments, nonreconstructible fragments, or impacted fragments, operative fixation is much less likely to produce a good result,15 and excision with or without prosthetic replacement is often preferable. Because most Mason type 3 fractures are associated with complex injury to the forearm or elbow, excision without replacement should be performed with caution and only in select patients.
Surgical Anatomy
The posterior interosseous nerve (PIN) is at risk of injury during approaches to the radial head due to its vulnerable location in the supinator muscle and its proximity to the radial neck. Pronation of the forearm translates the PIN away from the operative field approximately 1 cm anteromedially.42 With the forearm in pronation, the proximal 38 mm of the lateral aspect of the radius may be safely exposed (average proximal safe zone 52.0 ± 7.8 mm). Supination decreases the safe zone to 22 mm (average 33.4 ± 5.7 mm).43 Restricting dissection to within 4 cm from the radiocapitellar joint will protect the nerve from harm, regardless of forearm position.44 Displacement of diaphyseal fractures of the proximal radius results in a minimal effect of forearm rotation on PIN position. Also, proximal translation of the radius in Essex-Lopresti injuries is accompanied by proximal PIN migration in all forearm positions.45 Direct visualization and protection of the PIN might therefore be advisable when treating these injuries.
Surgical Technique
Video 17.1 Trans-olecranon Elbow Fracture Dislocation
Operative Exposures
For isolated fractures, exposure using Kocher′s interval between the anconeus and extensor carpi ulnaris is an option; however, the surgeon should not incise the capsule posterior to the anterior margin of the anconeus because this can damage the lateral collateral ligament (LCL) complex and lead to chronic posterolateral rotatory instability.12 The capsular incision should be made obliquely, in line with the original muscle interval. A more anterior interval such as that described by Kaplan46 and advocated by Hotchkiss47 involves splitting the common extensors, roughly between the extensor digitorum communis and the extensor carpi radialis brevis. Although this approach can better protect the LCL complex, it places the PIN at greater risk and can limit access to fragments that are displaced posteriorly in the elbow articulation.
Another approach to the radial head is the Wrightington approach.48 A posterior incision is made by elevating the anconeus from the ulna, and, rather than incising the insertion of the LCL complex, the crista supinatoris (the ridge where the ligament inserts) is osteotomized and later repaired. Because this approach does not affect the integrity of the LCL, compromise in the strength of the ligaments may be minimized.
When strict indications are applied, most radial head fractures that are surgically treated will be part of a fracture-dislocation of the elbow. In this situation, the LCL complex is nearly always avulsed from the lateral epicondyle, as are some of the common extensor muscles (Fig. 17.3). Furthermore, there is often a traumatic interval in the common extensor muscles that can be extended distally. In other words, it is easy to get excellent exposure of the radial head due to the associated ligament injury, and the surgical interval to use is defined by the injury.

When treating a posterior olecranon fracture-dislocation, there is often a posterior muscle injury that can be used to expose the radial head, particularly when the olecranon fragment is mobilized proximally to access the coronoid. One should limit dissection between the proximal radius and ulna to what occurred due to the injury itself, to reduce the potential for radioulnar synostosis.
When distal exposure is needed for plate fixation, the forearm should be pronated to protect the PIN. Blunt dissection of the supinator and identification of the PIN may be advisable in particularly complex cases.
Radial Head Excision
Radial head excision is straightforward. The surgeon merely creates a safe and adequate exposure and removes the fragments. The level of resection is kept at the junction of the radial head and neck when possible, in case a later reconstructive procedure is needed. If there is a LCL avulsion, it should be repaired.
Open Reduction and Internal Fixation
The techniques and prognosis of operative fixation of radial head fractures varies substantially depending on the type of fracture. Most isolated partial articular (Mason type 2) fractures have limited displacement. Wide displacement is usually associated with fracture-dislocation of the elbow. The fractured area is rotated into the muscle interval. In most cases the fragment is impacted, and the periosteal sleeve is intact. The fragment can be repositioned by elevating it with a bone tamp. This technique preserves a measure of the inherent stability associated with impacted fracture fragments. Provisional fixation with 0.035-inch Kirschner wires is exchanged for 2.0-mm screws. Interfragmentary screws are used only if there is thick, good-quality subchondral bone. Otherwise, compression of the fragment is applied with a bone clamp or manually, and position screws are inserted. Alternatively, variable-pitch headless screws can be used to provide compression.
Partial articular fractures associated with fracture dislocation are more likely to be completely displaced with little or no soft tissue attachment. They are also more likely to be comminuted. If there are missing fragments, fragments too small to secure, fragments with little or no subchondral bone, or very osteoporotic fragments, operative fixation may be difficult or impossible. In the setting of a fracture-dislocation of the elbow or forearm, even a partial articular fracture of the radial head may be an important stabilizing element, and accepting tenuous fixation may be unwise. For this reason we maintain a relatively low threshold for resecting the remaining radial head and replacing it with a prosthesis rather than accepting marginal fixation of a complex partial radial head fracture. If there are one or two large fragments with good-quality subchondral bone, they can be realigned and secured with screws. In many cases one or more fragments are impacted. In addition, bone fragments are often missing or impacted between the radial head fragments and the radial neck. In both situations, it may be useful to use a plate to buttress the repair.
Fractures involving the entire radial head (Mason type 3) are nearly always associated with a fracture-dislocation of the forearm or elbow. When the fracture is associated with a complete posterior dislocation of the elbow, wide exposure of the radial head is facilitated by the avulsion of the LCL complex from the lateral epicondyle (Fig. 17.3). When the LCL is not ruptured (e.g., Essex-Lopresti injury, radial head fracture with MCL injury), it may be necessary to detach the LCL origin and then repair it with a transosseous suture or suture anchors. Some surgeons prefer an osteotomy of the lateral epicondyle with direct bone-to-bone repair at the time of closure.49,50 In many cases it is easier to reassemble the articular fragments after they have been removed from the elbow wound and then replace the reconstructed radial head into the wound and secure it to the radial neck with a plate and screws. Small plates with 1.5- or 2.0-mm screws are used in most cases. In many cases a mini-condylar or blade plate is used. Some newer plate designs feature screws that lock to the plate, forming fixed-angle buttress pins. Bone grafting should be considered if there are areas of the neck with significant bone loss.
Plates and screws placed on the portion of the radial head that articulates with the sigmoid notch of the proximal ulna must be countersunk to limit impingement. A safe zone has been defined to allow insertion of hardware in the radial head. Based on anatomic studies, a 110-degree safe zone on the surface of the lateral aspect of the radial head may be mapped out during surgery.51 A horizontal reference mark is made first with the patient′s forearm in neutral position. Two more horizontal marks are then made with the patient′s forearm in full pronation and supination. The most anterior limit is defined as two-thirds the distance from the neutral to the fully supinated mark. The most posterior limit is one half the distance from the neutral to the fully pronated mark.
In general, if the safe zone is used, regular screws and plates should not impinge. In an anatomic study in which 2.0- or 2.7-mm T-plates were applied to the lateral aspect of the radial head with the patient′s forearm in neutral, there was no impingement with the sigmoid notch of the ulna.52 Alternatively, the region between the radial styloid and Lister′s tubercle is a useful guide for safe positioning of screws.9
A lag-screw technique is ideal to provide compression and increased stability but is not always possible. In the case of an isolated radial head fracture, one or more variable pitch countersunk, headless screws may be used.
Prosthetic Replacement
The radial neck is prepared with small reamers. A tight fit is not necessary. The size of the prosthesis is selected based on the resected fracture fragments. Prostheses that are too large can cause painful erosions of the capitellum and malalignment of the elbow (Fig. 17.4). Prostheses that are too small may provide inadequate stability. Oversizing of the prosthesis is more common, so it is safer to err toward a slightly smaller head. Using the largest fragment of the excised radial head as a template, a prosthesis with a slightly smaller diameter is selected. A prosthesis with a standard length is used in nearly every case. A pitfall is to measure the length of the head based on the largest radial head fragment. When that is done the prosthesis will sit on the proudest portion of the radial neck, equal to the shortest portion of the radial head. The level of resection should be the head–neck junction just as the neck begins to flare outward.

The radial head prosthesis acts as a stiff spacer. It does not need to have a tight fit in the intramedullary canal. It can be argued that a slightly undersized radial head and somewhat loose fit of the stem in the canal can accommodate the imperfect anatomy of the radial head compared with the native radial head. Another way to try to account for this is by using a radial head prosthesis with a mobile, bipolar head. The bipolar prosthesis requires resection of the radial neck to the biceps tuberosity and cement fixation—both of which are likely to be more difficult to salvage if problems occur.
Tips and Tricks
Isolated partial head fractures are the easiest fractures to fix but are the ones that need operative treatment the least. Protect the LCL, preserve the inherent stability of the fracture as you reduce it, and make sure the screws are not too long.
Many partial head fractures associated with fracture-dislocations are not reconstructible. Be prepared to replace the head with a prosthesis to ensure stability of the forearm or elbow.
Only fix fractures of the entire radial head with fewer than three fragments. There should be no missing fragments, no impaction or deformity of the fragments, and adequate subchondral bone. Do not hesitate to mobilize the LCL to improve exposure. Do not hesitate to remove minimal soft tissue attachments and extract the fragments from the wound to better manipulate them.
The major pitfall of radial head prosthetic replacement is overstuffing the joint. Err on the small side in the prosthetic sizing. The radial head should not extend beyond the lateral lip of the coronoid articular surface. The prosthesis does not have to have a tight fit in the intramedullary canal.
New Techniques
Several new plates and prostheses are in development. The plates incorporate locked buttress pins, which may help with support of the articular and metaphyseal fragments. The prostheses often incorporate a hinge for greater flexibility in anatomic contours.
Outcomes
Open Reduction and Internal Fixation
One retrospective review comparing open reduction and internal fixation versus nonoperative treatment of isolated Mason type 2 fractures of the radial head reported 90% good and excellent results for surgical treatment compared with 44% good and excellent results with nonoperative treatment. All of the fractures were Mason type 2 and were treated with screw fixation.33 This is contrary to our experience, in which the majority of Mason type 2 fractures recover very well without surgery, and long-term radiocapitellar arthritis is an uncommon source of problems or complaints in the office.
Duckworth et al4 reported 96% excellent or good results for nonoperative treatment of Mason type 2 fractures and found no significant difference in outcome between non-operative and operative treatment of Mason type 3 and 4 fractures.
Chen et al53 reported a direct comparison of internal fixation and radial head replacement of Mason type 3 fractures. They found excellent or good results in 90% with head replacement and 65% with internal fixation. The authors therefore concluded that radial head replacement is an appropriate option to best reconstruct stable structures of the elbow and avoid weakness, pain, and instability.
King et al23 reported in 1991 a direct comparison of internal fixation of Mason type 2 and 3 fractures. They found that isolated noncomminuted Mason type 2 fractures had 100% good or excellent results. Type 3 fractures had only 33% good or excellent results, prompting the authors to recommend excision or arthroplasty in the setting of radial head comminution.
Ring and colleagues15 found excellent results with operative treatment of isolated Mason type 2 fractures, but unsatisfactory results in four of 15 patients with Mason type 2 fractures associated with complex injuries. Among patients with Mason type 3 fractures with fewer than three articular fragments, two patients had nonunions (one of which eventually healed more than 2 years after the injury), and all patients had good forearm rotation. On the other hand, among patients with Mason type 3 fractures and three or more articular fragments, only one of 14 achieved a satisfactory result (three early failures, six non-unions, four poor forearm rotation).
Prosthetic Replacement
The use of a silicone prosthesis has lost favor due to fracture, dislocation, synovitis, lymphadenitis, and overall joint destruction.54 Replacement of the radial head with a metal or pyrocarbon implant has been associated with good short-and medium-term results in 70 to 82% of patients in spite of the frequent complexity of the overall injury.24,55–59 The long-term results are unknown. There is concern that articulation with a metal radial head will cause problems. It is now well recognized that an oversized prosthesis will cause early changes on the capitellum with pain, synovitis, and limitation of motion.
Pearls
The results of nonoperative treatment of isolated partial fractures of the radial head are generally very good. The indications for operative treatment of these injuries remain unclear.
Comminuted fractures of the entire head are nearly always associated with a fracture-dislocation of the forearm or elbow. Resection without replacement should be undertaken with great caution and only if the intraoperative exam shows no evidence of forearm or elbow ligament injury.
Retention of the native radial head is a worthwhile goal but only for relatively simple fractures (three or fewer fragments) where very reliable fixation can be obtained. Otherwise, prosthetic replacement should be considered, particularly in the setting of an Essex-Lopresti lesion or a terrible triad fracture-dislocation of the elbow in which radiocapitellar contact is critical to a good outcome.
Complications
Nonunion of radial head fractures can occur with both non operative and operative treatment. In both cases the nonunions are usually associated with limited or no symptoms, and late healing can occur. Crepitus and pain related to the hardware often lead to a second surgery for radial head excision.
Loss of motion related to a malunited fracture of the radial head can often be salvaged with resection of the radial head.
Simple Elbow Dislocations
The elbow joint is inherently stable but dislocates at a rate second only to the shoulder, reflecting its vulnerability to injury.60,61 Although most of the capsuloligamentous structures must be disrupted for a dislocation to occur,62 the majority of patients do not experience a redislocation in the absence of associated fractures.63,64 Dislocations of the elbow without associated fractures have been referred to as simple elbow dislocations, with fracture-dislocations representing complex dislocations.
Classification
The majority of elbow dislocations and fracture-dislocations result in injury to all of the capsuloligamentous stabilizers of the elbow joint.62,65–67 The exceptions include fracture-dislocations of the olecranon and other injuries with fractures of the coronoid involving nearly the entire coronoid process; these fractures are so unstable that elbow dislocation may occur despite less soft tissue injury.1,32,68,69
The progression of capsuloligamentous injury during elbow dislocation progresses from lateral to medial, and the elbow can completely dislocate with the anterior band of the MCL intact (Fig. 17.5).62 There is also a variable degree of injury to the common flexor and extensor musculature.60,65,67,70–72 One study notes that the LCL complex fails by avulsion from the lateral epicondyle in over 75% of patients with elbow dislocations (Fig. 17.3).73 In our observations in treating over 60 fracture-dislocations of the elbow, we have found that the LCL is always avulsed from the lateral epicondyle. In many patients there are small pieces of the ligament or other long strands of musculotendinous tissue, which may lead the surgeon to misinterpret the situation (Fig. 17.3). Defined practically, reattachment of the soft tissue sleeve to the lateral epicondyle is nearly always sufficient.

Considerations of the direction of dislocation of the elbow are of limited value. Anterior dislocations are rare. Medial and lateral dislocations probably represent incompletely reduced posterior dislocations. Nearly all dislocations are posterior in direction. There is no established value to distinguishing posteromedial and posterolateral dislocations, although a posteromedial dislocation might be associated with a relative sparing of the medial soft tissues.61,62
O′Driscoll et al62 described several stages of elbow instability. Stage 1 involves partial or complete disruption of the LCL, which may result in slight posterior subluxation of the radial head with respect to the capitellum. Stage 2 involves an incomplete posterior dislocation with disruption of the lateral ligamentous complex and further injury to the osseous or ligamentous supporting structures either or both anteriorly and posteriorly. The medial edge of the ulna may be found to rest on the trochlea. This gives the appearance of the coronoid perched on the trochlea on a lateral radiograph. Stage 3 is divided into three subgroups, A through C. Stage 3A involves injury to all the soft tissue support except the anterior band of the MCL. The elbow dislocates in a posterolateral direction rotating about the intact anterior MCL. Stage 3B involves injury to the entire medial ligamentous complex resulting in varus, valgus, and rotary instability. Stage 3C injuries are very unstable due to complete soft tissue disruption from the distal humerus, with the ability to dislocate even when immobilized in a cast.1
Nonoperative Treatment
Nonoperative treatment is preferable for all simple elbow dislocations, with operative treatment reserved for the unusual patient with persistent instability after manipulative reduction and active exercise. Manipulative reduction can usually be obtained in the emergency room with the patient under conscious sedation. When the elbow has been dislocated for a long period of time, general anesthesia or regional block may be preferable. On occasion, very unstable dislocations that are seen acutely (for instance, an athlete on the playing field, or an older person with extensive muscle injury) may be reduced without anesthesia.
During manipulative reduction, it is important to keep the patient′s elbow in a relatively flexed position to limit the potential for entrapment of the median nerve and brachial artery within the joint. Usually, the alignment of the patient′s forearm in the medial-lateral plane is corrected first, and then the elbow is reduced with anteriorly directed pressure over the olecranon, supination of the forearm, and longitudinal traction. It can be helpful to perform the reduction with the patient in the lateral decubitus or prone position when an assistant is not available to provide countertraction on the patient′s upper arm.
Anatomic landmarks can be palpated to assess the alignment of the elbow prior to splinting and postreduction radiographs. The medial and lateral epicondyles and the dorsal point of the olecranon should form a triangle in the coronal plane. If the point of the olecranon is still posterior to the epicondyles, the elbow may not be concentrically reduced.
After manipulative reduction, testing of varus and valgus instability will not influence management. One should expect to find valgus instability unless this is one of the uncommon dislocations with incomplete MCL injury. Varus instability is more difficult to isolate.74 For the same reason, there is no point in performing a test for posterolateral rotatory instability (so-called pivot shift of the elbow11); one would expect it to be positive in 100% of adequately relaxed elbows, and it would not alter management.
It is more important to determine if there is a tendency for the elbow to subluxate or re-dislocate as the elbow is extended and at what point this occurs. If the elbow re-dislocates prior to ~ 30 degrees of flexion, retest it with the forearm in full pronation. Some surgeons have suggested that if this maneuver restores stability, a hinged brace that holds the forearm pronated may be useful.75,76 Others recommend a hinged brace that prevents extension beyond the point of stability for a few weeks.75 Our experience has been that an unstable elbow can dislocate in a cast,77 and the patient may not be aware of it; therefore, we do not trust fracture braces and consider surgical treatment of elbows that re-dislocate prior to near-terminal extension.
The patient is splinted for 1 or 2 weeks for comfort. The position of immobilization is usually 90 degrees of elbow flexion and neutral forearm rotation, although the forearm is pronated on occasion. Splinting for more than 2 weeks is associated with greater pain and stiffness.63,64,71 In motivated patients it is not necessary to splint the elbow after dislocation.78
Patients should be seen by an orthopaedic surgeon within 2 weeks and encouraged to use their arm for light functional activity. They are taught exercises for regaining motion. Some patients have a slight residual malalignment of the elbow demonstrated on radiographs (Fig. 17.6).67,79–81 Our preference is to treat this with a 1-week trial of confident active exercises because this finding often represents a type of “pseudosubluxation” related to muscle relaxation from pain similar to that observed in shoulders. If addition of the dynamic muscular component of elbow stability fails to restore alignment, or if there is an associated coronoid fracture, surgical treatment may be necessary.

Surgical Treatment
Indications
In general, there are two types of patients in whom it may prove difficult or impossible to maintain a concentric reduction of a simple elbow dislocation: younger patients with very high energy dislocations (such as a fall from several stories), and older patients after simple falls. Both mechanisms involve more extensive avulsion of the muscle origins along with the capsuloligamentous structures.72
Surgical Anatomy
In some older patients, the medial muscular attachments to the humerus may be relatively spared, causing the elbow to hinge open due to more extensive disruption of the muscles and ligaments on the lateral side (Fig. 17.7). The majority of patients with unstable simple elbow dislocations have extensive injury to the muscles that originates from the distal humerus.

Surviving the Night
On occasion an elbow dislocation or fracture-dislocation is associated with brachial artery injury requiring emergent interposition vein graft, particularly dislocations with a large medial wound. The presence of a distal pulse is not a reliable indicator of vascular integrity because of the excellent longitudinal collateral arterial circulation in the arm. Therefore, vigilance is warranted in high-energy injuries.
Elbow dislocations associated with displaced, unstable forearm or wrist injuries are at high risk for compartment syndrome. An elbow that will not stay reduced is not an emergency and can be splinted and treated during the next week.
Surgical Techniques
Soft Tissue Repair
Older patients with unstable simple elbow dislocations that seem to rotate out of joint on a relatively spared medial soft tissue hinge are usually easily stabilized by reattaching the LCL complex and common extensor musculature to the lateral epicondyle (Fig. 17.8). If repair of the lateral soft tissue stabilizers alone proves insufficient, a medial exposure can be performed, the ulnar nerve subcutaneously transposed, and the MCL and flexor-pronator muscle mass reattached to the medial epicondyle (Fig. 17.8c,d). These repairs can be performed either with suture anchors or with drill holes placed through bone. The origin of the LCL should be reattached as close as possible to its anatomic location at the center of rotation of the elbow—at the inferior point of a small tubercle on the lateral epicondyle. The origin of the MCL should be reattached to the inferior surface of the medial epicondyle. The common flexor and extensor musculature is attached at these points and more proximal as needed.

Cross-Pinning of the Joint
In an older, infirm patient with limited demands and high anesthesia risk, a closed manipulation and cross-pinning of the elbow joint can be sufficient. Two stout, smooth Kirschner wires are used, avoiding the medial side of the elbow and the ulnar nerve. Some surgeons prefer to use screws due to concern that the Kirschner wires might not be strong enough, but we have not had any problem with wires for this particular indication. The pins are protected with an above-elbow cast. The pins are removed and the cast discontinued 4 weeks later (Fig. 17.9).

Hinged External Fixation
In younger patients with high-energy injuries, repair of the medial and lateral collateral ligaments is sometimes insufficient.72,82 It is important to be prepared to either cross-pin the joint or apply a hinged external fixator (Fig. 17.10). We prefer to use hinged external fixation and allow the patient to move because immobilizing the elbow may increase the already substantial risk of heterotopic ossification; however, stability always takes precedence over mobility in the treatment of elbow problems, and if a surgeon does not have the resources or technical ability to apply a hinged external fixator, cross-pinning may be used.

Determination of the isometric center of rotation at the elbow is critical to the use of a hinged external fixator. A temporary axis pin is placed in the distal humerus through the center of rotation. This roughly corresponds to a point on the medial aspect of the trochlea just anterior and inferior to the medial epicondyle and to the distalmost point of a small ridge on the lateral epicondyle in the center of the capitellum. Proper axis pin placement is confirmed with imaging. The frame is usually attached to the humerus first and then to the forearm.
Several types of hinges are available. The Compass Hinge (Smith & Nephew Inc., Memphis, TN) may provide additional stability by virtue of both posteromedial and posterolateral pins. It also incorporates a worm gear that can be used to assist with motion during the initial painful postoperative period and can be used for static progressive stretch later on in the rehabilitation. The majority of other fixators are unilateral, although some can be used with transfixion pins if additional stability is desired. A lateral-only frame avoids the discomfort associated with a medial frame and pins, and usually provides adequate stability. No matter what fixator is used, the lateral humerus pins must be placed with an open exposure adequate to protect the radial nerve.
Tips and Tricks
Many surgeons repair the collateral ligaments and common flexor and extensor muscles using drill holes through bone. The potential advantages include broader contact between soft tissues and bone and more reliable fixation in poor quality bone. We believe that suture anchors simplify the repair, and we continue to use them in most patients.
Application of a hinged external fixator is challenging. To simplify the procedure, stabilize the ulnohumeral joint in good alignment with one or two stout, smooth Kirschner wires while the hinge is applied.
We always make a more substantial incision for the lateral humerus pins (at least 2 inches). We then dissect down to bone and use small Hohmann retractors to ensure that the radial nerve is safe. We have yet to have a radial nerve palsy or injury in over 20 hinge applications.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


