Embroyology and congenital anomalies of the hepatobiliary system
9.6: Embroyology and congenital anomalies of the hepatobiliary system
Janani Kalyanraman, Janani Baradwaj
Introduction
The hepatobiliary system comprises of the liver, gallbladder and extrahepatic biliary apparatus, pancreas and spleen.
Liver
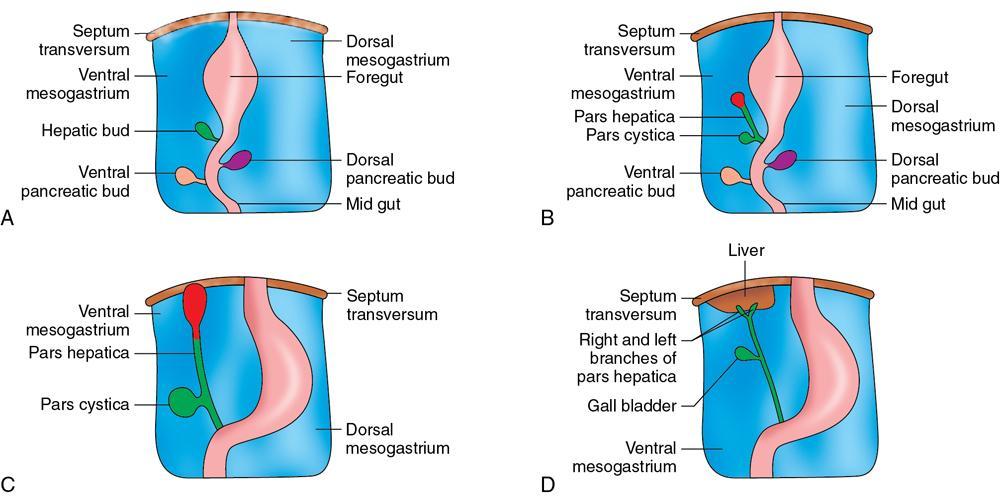
The liver develops from an endodermal bud during the fourth week of intrauterine gestation that arises from the ventral aspect of the terminal part of foregut (future second part of duodenum).
This bud grows into the ventral mesogastrium and passes through it into the septum transversum (unsplit part of intraembryonic mesoderm between the pericardial cavity and the yolk sac cavity that has an inductive effect on differentiation, proliferation, branching and formation of hepatocytes and cells lining the intrahepatic and extrahepatic biliary apparatus from the hepatic bud).
The hepatic diverticulum or bud then enlarges and divides into two parts: The larger cranial portion becomes the hepatic primordium/pars hepatica and the smaller caudal portion (pars cystica) expands to form the gallbladder and its stalk, the cystic duct.
Pars hepatica
The endodermal cells of the hepatic bud give rise to parenchyma of the liver and biliary capillaries (Fig. 9.6.1). The mesoderm of the septum transversum forms the capsule and fibrous tissue of the liver along with haematopoietic tissue and Kupffer cells.
1. Hepatic lobes: The liver grows rapidly and soon fills up most of the abdominal cavity. Initially, the right and left lobes of the liver are equal in size, eventually the right lobe becomes larger and the caudate and quadrate lobes develop as subdivisions of the left lobe.
In the 12 weeks of intrauterine gestation, the weight of liver is one-tenth of the total body weight of foetus and occupies most of the upper abdomen and by the 28–30 weeks, it reduces to one-fifth of the body weight. (Attributed to the oxygen rich blood supply through the left umbilical vein and ductus venosus, presence of large number of sinusoids and rapidly proliferating haemopoietic tissue. Further facilitated by herniation of midgut between the sixth and tenth weeks of intrauterine gestation.)
2. Hepatic architecture: As the terminal branches of the pars hepatica reach septum transversum, the cells arising from them are broken up into interlacing columns called hepatic trabeculae. In between hepatic trabeculae, the hepatic sinusoids develop in situ.
3. Hepatic sinusoids: As the cords penetrate the septum transversum, they cause fragmentation of the umbilical and vitelline veins that supply the liver, resulting in the formation of the hepatic sinusoid network.
Reorganization of cells of hepatic bud and the mesenchymal cells of connective tissue and blood vessels form the hepatic lobule with bile canaliculi, portal triad and sinusoids of liver.
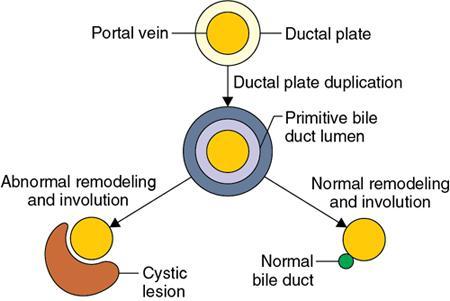
4. Intrahepatic biliary radicle (IHBR): Ductal plate is defined as a double-layered cylindrical structure (Fig. 9.6.2) of the bile duct epithelium that surrounds the portal ramifications by the eighth gestational week. Later by the twelfth gestational week, remodelling of ductal plate begins, and maturity is attained by the end of gestation or early postnatal period. Within the substance of liver, the hepatic ducts branch repeatedly and canalized to acquire a lumen to form IHBRs.
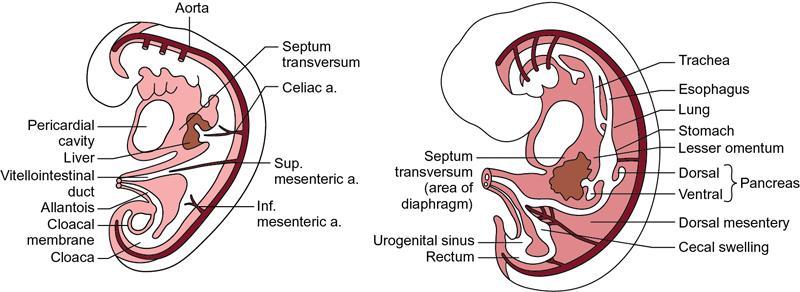
5. Peritoneal folds in relation with the liver: With the rapid growth of developing liver into the septum transversum, the mesoderm of septum transversum between the liver and the foregut becomes the lesser omentum (Fig. 9.6.3), and the part between the liver and the ventral abdominal wall becomes the falciform, triangular and coronary ligaments. Lesser omentum and falciform ligament together are called ventral mesentery/ventral mesogastrium.
Fig. 9.6.1Sequence of the formation of the liver and the bile ducts. (A) Formation of the hepatic bud from the ventral aspect of the terminal part of foregut. (B) Division of the hepatic bud into two. (C) Extension and migration of the liver toward the septum transversum. (D) The enlargement and division of the liver.
Fig. 9.6.3Sagittal section of the illustrated embryo depicting the relationship of liver with the adjacent peritoneal structures.
Portal vein
• The portal vein is derived from the right and left vitelline veins and anastomoses between them. (Vitelline veins/omphalomesenteric veins arise from the yolk sac.)
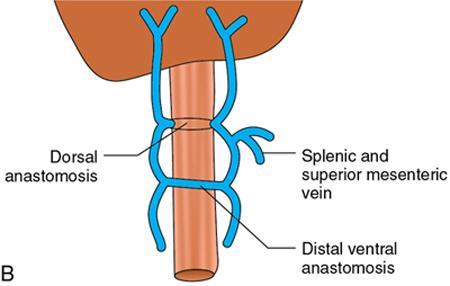
• The infrahepatic/proximal parts of the two vitelline veins lie on either sides of the developing duodenum (Fig. 9.6.4A).
• Three transverse anastomoses interconnect the vitelline veins, two of which lie ventral to the duodenum. The third anastomosis lies dorsal to the duodenum, and is between the two ventral anastomoses forming a figure of eight around the duodenum (Fig. 9.6.4B).
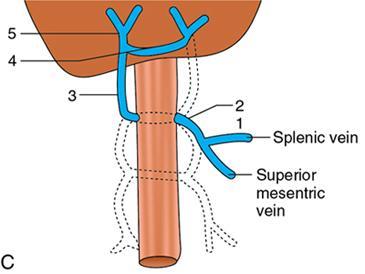
• The superior mesenteric vein (SMV) and splenic vein (which develop independently) join the left vitelline vein, a short distance caudal to the dorsal anastomosis.
• Some parts of the vitelline veins now disappear. The portal vein and its right and left divisions are derived from the veins that remain (Fig. 9.6.4C).
• Thus the portal vein is formed from Fig. 9.6.4C:
1. Part of left vitelline vein.
2. Dorsal anastomosis.
3. Part of right vitelline vein.
4. The cranial ventral anastomosis becomes the left branch of the portal vein.
5. Right vitelline cranial to cranial ventral anastomosis forms right branch.
Fig. 9.6.4(A) The vitelline veins lie on the left and right of the duodenum. (B) Figure of eight formation by the transverse anastomosis between the vitelline veins, ventral anastomosis superiorly and inferiorly and dorsal anastomosis in between. (C) Splenic vein and SMV join the left vitelline vein at the level of the dorsal anastomosis. Formation of the final portal vein: (1) Part of left vitelline vein, (2) dorsal anastomosis, (3) part of right vitelline vein, (4) the cranial ventral anastomosis becomes the left branch of the portal vein and (5) right vitelline cranial to cranial ventral anastomosis forms right branch.
Hepatic vein
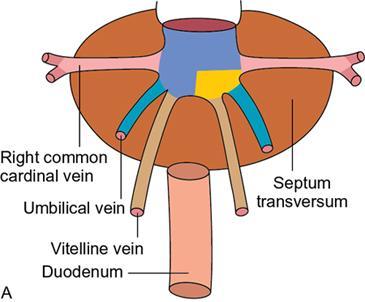
• With the appearance of hepatic bud in septum transversum, the vitelline veins can be divided into three parts: Intrahepatic part, suprahepatic part and infrahepatic part.
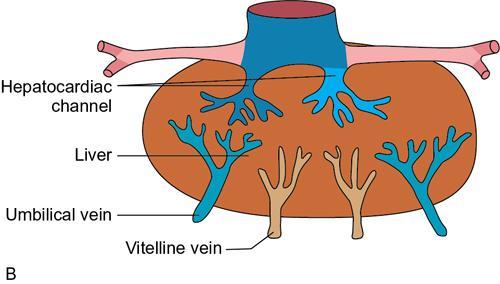
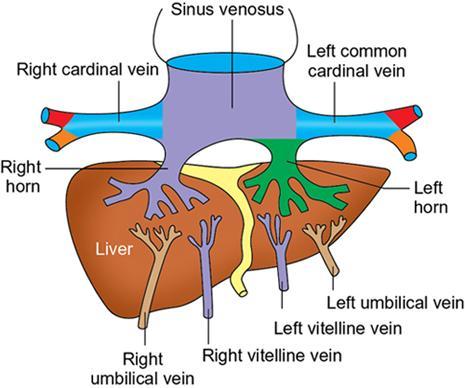
• The hepatic sinusoids drain into the sinus venosus (Fig. 9.6.5A), through the right and left hepatocardiac channels (which are the persisting terminal parts of the vitelline veins).
• The proximal parts of the umbilical veins lose their communications with the sinus venosus (Fig. 9.6.5B).
• At the same time, hepatocardiac channel disappears as the left horn of the sinus venosus undergoes retrogression.
• The blood from the umbilical and vitelline veins are channelized to the right hepatocardiac channel (common hepatic vein [CHD]) which forms the cranial most part of the inferior vena cava (IVC) (Fig. 9.6.5C).
• Similarly, the right umbilical vein disappears and all blood from the placenta reaches the developing liver through the left vein (Fig. 9.6.5D).
• In order to facilitate the passage of this blood through the liver, some of the sinusoids enlarge to create a direct passage connecting the left umbilical vein to the right hepatocardiac channel. This passage is called the ductus venosus (Fig. 9.6.6).
Fig. 9.6.5(A) The umbilical veins (UVs) and vitelline veins (VVs) passing through the septum transversum to reach the sinus venosus. (B) Growth of liver cells within the septum transversum breaks up part of the UV and VV into capillaries. Blood reaching the liver through the UV and VV now goes to the heart through the right and left hepatocardiac channels. (C) Left hepatocardiac channel disappears. (D) Right hepatocardiac channel (which later forms part of the IVC) now drains the liver. Right umbilical veins disappear. All the blood from the placenta now reaches the liver through the left umbilical vein. Formation of ductus venosus short-circuits the blood to the right hepatocardiac channel.
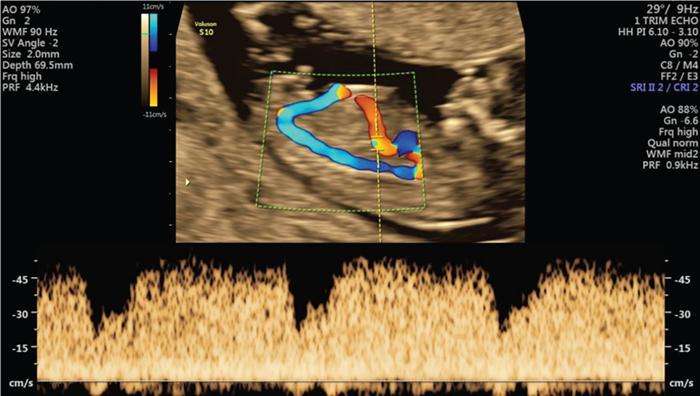
Fig. 9.6.6Ductus venosus: Classical triphasic waveform where the flow should be in the forward direction, directed to the heart.
Anomalies of the liver
1. Absence of quadrate lobe.
2. Agenesis of the hepatic lobes; left hepatic lobe > right hepatic lobe.
3. Riedel’s lobe (Fig. 9.6.7): Tongue-like extension of the right lobe of the liver.
4. Sliver of the liver (Fig. 9.6.8): Left lateral extension of the left lobe of the liver, which appears as a crescentic structure wrapping around the lateral aspect of the spleen, otherwise known as the beaver tail of liver.
5. Anomalous lobulation. (Can be confused for cirrhotic liver, hence must be assessed with caution.)
6. Papillary process of the caudate lobe (Fig. 9.6.9).
8. Accessory fissures and diaphragmatic slips (Fig. 9.6.11).
9. Intrahepatic biliary atresia: It is a serious anomaly and is not compatible with life unless a liver transplantation is undertaken, which is characterized by an absence or severe deficiency of the extrahepatic biliary tree that results in idiopathic destructive inflammatory process which leads to fibrotic remnants at porta hepatis.
It is of two types: Isolated/nonsyndromic and syndromic, which is associated heterotaxy syndrome/asplenia/polysplenia/interrupted IVC and malrotations.
Classified by Kasai classification:
• Type I: Obliteration of common bile duct (CBD) (patent cystic duct and CHD).
• Type II:
IIa: Obliteration of CHD (patent cystic duct and CBD), sometimes with a cyst at hilum, hence termed cystic biliary atresia.
IIb: Obliteration of CHD, cystic duct and CBD.
• Type III: Obliteration of left and right main hepatic ducts at the level of porta hepatis (most common, 90%).
USG findings (Fig. 9.6.12A and B): Echogenic fibrous tissue anterior to the portal vein: Triangular cord sign.
Larger hepatic arterial calibre (right proximal hepatic artery diameter >1.5 mm and hepatic artery to portal vein diameter ratio >0.45) with subcapsular hepatic arterial flow on Doppler.
Gallbladder ghost triad and decreased gallbladder contraction index for age (Fig. 9.6.12C).
Colour Doppler (Fig. 9.6.13): Hepatic arterial flow extending to the hepatic surface – subcapsular telangiectasia.
Gold standard test: Hepatobiliary iminodiacetic acid (HIDA) scan (Fig. 9.6.14): Shows relatively good hepatic uptake with no evidence of excretion into the bowel at 24 h.
10. Rudimentary liver.
11. Ductal plate malformation: Multifocal cystic dilatation of segmental intrahepatic bile ducts as a result of ductal plate malformation. Dilatation depends on the level of the biliary tree that is affected (Fig. 9.6.15).
• Biliary hamartoma: Disorganized clusters of dilated cystic ductal plate remnants that have failed to involute (Fig. 9.6.16).
• Congenital hepatic fibrosis: Variable degree of periportal fibrosis with irregularly shaped proliferating bile ducts (Fig. 9.6.17). Manifests as fibropolycystic disease. Biliary hamartomas, Caroli’s disease, polycystic liver disease and choledochal cysts often coexists.
• Polycystic liver disease: Failure of union of intrahepatic biliary canaliculi and ductules with extrahepatic bile ducts, results in the formation of cysts within the liver. It is usually associated with cysts in the kidney and pancreas (Fig. 9.6.18).
• Caroli’s disease (the simple type): Incomplete ductal plate remodelling resulting in persistent abnormal ductal plate remnants involving the large bile ducts.
• Caroli’s syndrome (the periportal type of Caroli’s disease): Both the ductal plates and central intrahepatic bile ducts of the smaller peripheral bile ducts are affected, with the former leading to the development of fibrosis.