Embryonal tumors of the central nervous system (CNS) are poorly differentiated, mitotically active, histologically and clinically aggressive, and highly cellular neoplasms and constitute the most common group of malignant brain tumors in children. Commonly referred to as small round blue cell tumors, the embryonal tumor group includes medulloblastoma, embryonal tumor with multilayered rosettes, atypical teratoid/rhabdoid tumor, CNS neuroblastoma, and high-grade neuroepithelial tumor with BCL-6 co-repressor (BCOR) internal tandem duplication as well as a spectrum of other CNS embryonal tumors that were previously called CNS primitive neuroectodermal tumors.
Subtype
Age
Histology
Molecular/genetic mutations
Prognosis
Medulloblastoma
WNT-activated
Children, teens
Classic
Large cell/anaplastic
CTNNB1, TP53, SMARCA4, DDX3X
Favorable
SHH-activated, TP53-mutant
Infants, adults
Large cell/anaplastic
Desmoplastic/nodular
ATOH1, PTCH1, TP53 germline
Very poor
SHH-activated, TP53-wildtype
Infants, adults
Large cell/anaplastic
Desmoplastic/nodular
Extensive nodularity
ATOH1, PTCH1, TP53-wildtype
Intermediate to Poor
Non-WNT/non-SHH group 3
Infants, children
Classic
Large cell/anaplastic
MYC, SMARCA4, OTX2, CTDNEP1, LRP1B
Poor
Non-WNT/non-SHH group 4
Infants, children, adults
Classic
Large cell/anaplastic
KDM6A 17p deletion, 17q gain
Poor
Embryonal tumor with multilayered rosettes (ETMR)
0-4 yrs
Small cells forming multilayered rosettes, fibrillary zones; LIN28+
C19MC-altered at chromosome 19q; chromosome 2 gain
Poor
Atypical teratoid/rhabdoid tumor (ATRT)
<3 yrs
Spindle-shaped cells clustered in papillary or trabecular pattern
SMARCB1 locus at 22q11.2
Very poor
CNS neuroblastoma
4 wks-20 yrs
Zones of neurocytic differentiation & densely packed primitive embryonal cells
FOXR2 NKX2-1 1p gain
Poor
High-grade neuroepithelial tumor with BCOR internal tandem duplication (HGNET-BCOR-ITD)
7 mos-22 yrs
Spindle to oval cells with fine chromatin, microcystic features, perivascular pseudo-rosettes, fibrillary cytoplasmic processes
Somatic internal tandem duplications in the 3rd end (exon 15) of BCOR gene
Poor
BCOR, BCL-6 co-repressor.
Medulloblastoma
Definition: Medulloblastoma is the most common embryonal neuroepithelial tumor arising in the cerebellum or posterior brain stem and most common malignant tumor of childhood consisting of densely packed small and round undifferentiated cells with high mitotic count.
Epidemiology: This is the most common CNS embryonal tumor of childhood and the second most common pediatric brain tumors after pilocytic astrocytoma; it accounts for up to 25% of all intracranial neoplasms in children. The median age at diagnosis of medulloblastoma is 9 years, with peaks incident at 3 and 7 years of age; it is more common in boys, with female-to-male ratio of 1:1.7. Among patients aged >3 years, the female-to-male ratio is 1:2. The various molecular groups and histopathological variants of medulloblastoma have different age distributions.
Molecular and genetic profile: Medulloblastomas are divided into four distinct molecular subtypes based on molecular profiles: WNT-activated, sonic hedgehog (SHH)-activated, non-WNT/non-SHH-activated group 3, and non-WNT/non-SHH-activated group 4.
Clinical features and standard therapy
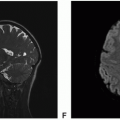
Figure 11.1. Imaging of medulloblastoma, WNT-activated. A-C. Axial T2: Heterogeneously isointense mass in the right cerebellopontine angle with posterior cystic components with fluid-fluid level. D. Axial diffusion-weighted imaging (DWI): Mildly hyperintense signal within the solid component. E. Axial apparent diffusion coefficient (ADC): Mildly reduced diffusion within the solid component. F. Coronal fluid-attenuated inversion recovery (FLAIR): Heterogeneously isointense mass.
Figure 11.1.(continued)G. Axial FIESTA: Heterogeneously isointense mass in the right cerebellopontine angle with posterior cystic components with fluid-blood levels. H. Axial T1 precontrast: Homogeneously hypointense signal within the solid component. I. Axial T1 postcontrast: Avid enhancement within the solid component.
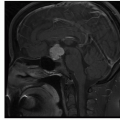
Figure 11.2. Imaging of medulloblastoma, SHH-activated. A-C. Axial T2: Heterogeneously slightly hyperintense solid mass in the left cerebellum. D-F. Sagittal T2: Slightly hyperintense solid mass with mild surrounding edema.
Figure 11.2.(continued)G-I. Coronal FLAIR: Slightly hyperintense solid mass with mild surrounding edema. J-L. Axial DWI: Markedly reduced hypercellular mass.
Figure 11.2.(continued)M-O. Axial T1 precontrast: Hypointense mass. P-R. Axial T1 postcontrast: Avid enhancement within the mass.
Figure 11.2.(continued)S-U. Sagittal T1 postcontrast: Avid enhancement within the mass and effacement of fourth ventricle due to mass effect.
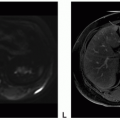
Figure 11.3. Imaging of medulloblastoma, non-WNT/non-SHH-activated, group 3. A. Sagittal T1 precontrast: Homogeneously hypointense midline mass. B. Sagittal T2: Heterogeneously hypointense mass. C. Coronal FLAIR: Mildly hyperintense mass with areas of cystic component and moderate surrounding edema. D. Axial DWI: Hyperintense mass. E. Axial ADC: Hypointense mass with reduced diffusion due to hypercellularity. F. Coronal ADC: Hypointense mass with reduced diffusion due to hypercellularity.
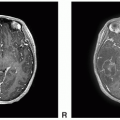
Figure 11.3.(continued)G-I. Axial T1 postcontrast: Avid enhancement of the dominant solid tumor with small peripheral cystic components. J. Sagittal T1 postcontrast: Multilobular contour of the mass with avid enhancement. K-L. Coronal T1 postcontrast: Multilobular contour of the mass with avid enhancement with small peripheral cystic components.
Only gold members can continue reading. Log In or Register to continue