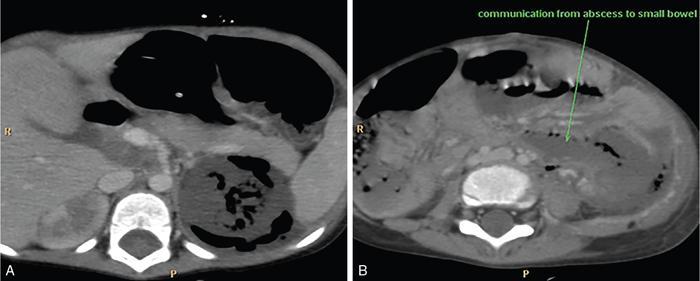
It is a rare necrotizing infection of kidneys with abnormal accumulation of air within parenchyma, pelvicalyceal system and in perinephric soft tissue. If not treated early, it can lead to morbid sepsis. Adult females are commonly affected. It tends to affect patients with uncontrolled diabetes, urinary tract obstruction, immunocompromised individuals, neoplasms or sloughing of papilla. Presenting complaints are fever, chills, flank pain, nausea and vomiting. Leucocytosis, raised white blood cell count, ESR, C-reactive protein, hyperglycaemia, acidosis, dehydration and electrolyte imbalance are prominent findings. Glucose fermenting bacteria such as E. coli (most common), Klebsiella, Pseudomonas and Proteus mirabilis are the causative organisms. Proteus, Aerobacter and Candida are additional causative organisms. Air is visualized as mottled lucencies within the renal fossa or crescentic collections of gas within the Gerota’s fascia. On grey scale imaging, there may be nonvisualization of the kidney due to air. Dirty echogenic foci with reverberation/ring-down artefacts representing gas (‘dirty shadowing’) in renal parenchyma, pelvicalyceal system and perinephric soft tissue are also seen. Renal enlargement may be seen. CTU is the most accurate and diagnostic modality. Kidneys appear enlarged and show destruction of renal parenchyma with accumulation of air in the parenchyma pelvicalyceal system and perinephric soft tissue (Fig. 10.12.2.2.1).
2. Emphysematous pyelonephritis
Epidemiology
Clinical features
Lab parameters
Pathology
Imaging
Plain radiograph and IVP
USG
CECT
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


