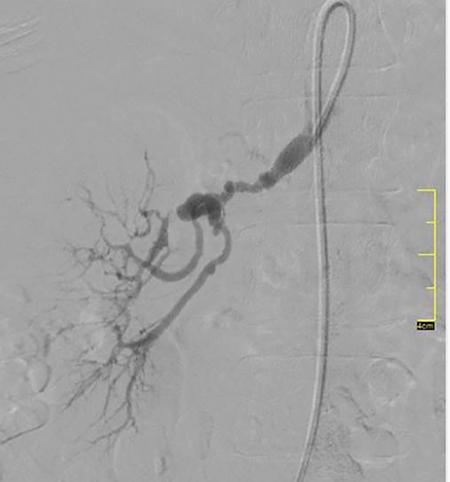
Vikash Jain Renal artery stenosis (RAS) may result in refractory hypertension, progressive renal insufficiency and cardiovascular complications such as refractory heart failure, flash pulmonary edema and acute coronary syndrome. There is overwhelming evidence that hypertension associated with a haemodynamically significant atherosclerotic RAS is better controlled with fewer medicines following renal revascularization. A meta-analysis of small series indicated that renal function is improved in about 30% and stabilized in 38% with an overall favourable response of 68% following percutaneous transluminal renal angioplasty (PTRA) in atherosclerotic renal artery stenosis (ARAS). Several randomized controlled trials have shown no difference in outcomes with optimal medical therapy (OMT) and PTRA compared with OMT alone in terms of BP control, preservation of renal function or major cardiovascular events. However, each of these trials had significant design flaws that ranged from variability in inclusion and exclusion criteria, inconsistent definitions of improvement that limit their applicability in day to day practice, making the selection of patients for renal artery stenting a controversial topic. These trials excluded patients with resistant hypertension, accelerated hypertension, advanced kidney disease, history of refractory heart failure or a recent acute coronary syndrome. This patient group who was most likely to be benefitted by PTRA was excluded in the trials. Atherosclerosis is the most common cause (90%) of RAS in adults, with fibromuscular dysplasia (FMD) being more common in younger female patients. ARAS is the most common cause of secondary hypertension affecting 25%–35% of the patients with secondary hypertension. Approximately 25% of elderly patients with chronic kidney disease (CKD) were found to have unsuspected ARAS. In elderly population referred for coronary angiography and having coexistent hypertension, haemodynamically significant RAS (>70%) was found in more than 20% of patients. FMD is a nonatherosclerotic, noninflammatory, congenital condition that leads to dissection, aneurysm or stenosis of medium-sized artery predominantly affecting renal, carotid and femoral. It usually involves mid to distal portion of the renal artery. On angiography, FMD shows characteristic ‘string of pearls’ appearance or less commonly concentric smooth stenosis (Fig. 10.20.1). Renal FMD has a female preponderance, and can lead to HTN, which is preferentially treated with balloon angioplasty. CLINICAL FINDINGS ASSOCIATED WITH RENOVASCULAR DISEASE
10.20: Endovascular management of renal artery stenosis
Introduction
Clinical manifestation of RAS
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Endovascular management of renal artery stenosis