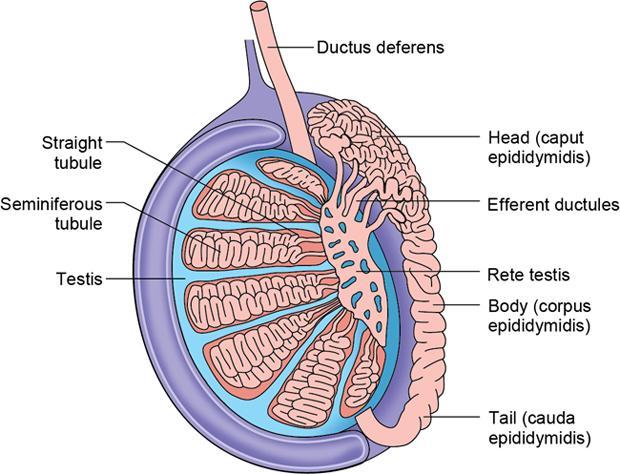
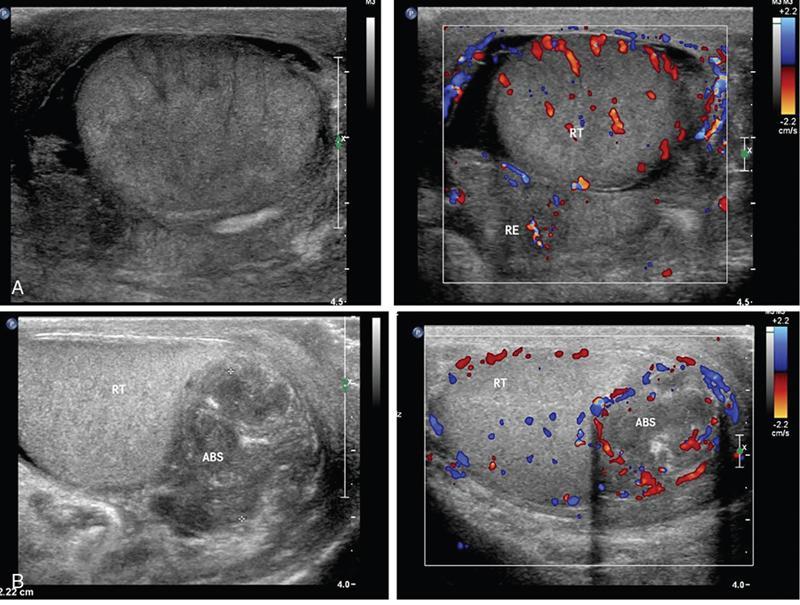
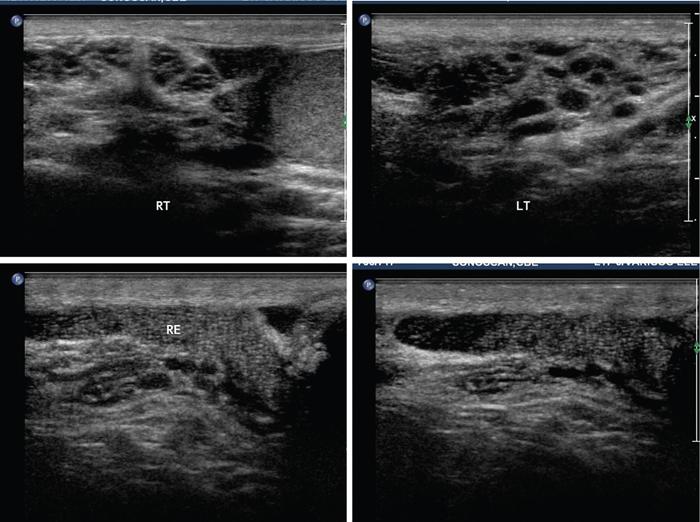
Bobji Kettay The epididymis is positioned in the posterolateral aspect of testis and subdivided into three parts namely, the head, body and tail. Collection and temporary storage of sperms till maturation are its functions. The tail of epididymis continues as the vas deference (Fig. 11.9.1). The epididymis is ideally imaged with USG using a high frequency (7.5 to 10 MHz), linear array, near focused transducer and is best viewed in the longitudinal plane. Its echogenicity is similar to that of testis but echotexture is coarser than testes (Fig. 11.9.2). MRI is a complimentary modality. Epididymis appears slightly heterogeneous and is isointense to testicular parenchyma on T1WI. On T2WI, it shows slightly reduced intensity than testis. Retrograde (ascending) bacterial infection from lower urinary tract is the commonest cause for epididymitis. In sexually active men, <35 years of age, Neisseria gonorrhoea and Chlamydia trachomatis are the causative agents. Escherichia coli is the cause in children and >35 years old. Tail of epididymis is first to get affected because of the ascending nature of the infection. So thorough evaluation of the tail during USG is essential to diagnose the early stage of the disease. Body and head are subsequently involved and the infection can also spread to the testis. Noninfective acute epididymitis is called as chemical epididymitis. This occurs when sterile urine is extravasated into epididymis due to increased intraabdominal pressure during acts like straining. Chemical epididymitis spares the head and affects only the tail of epididymis. Patients present with scrotal swelling, pain, pyuria and fever.
11.9: Epididymis
Imaging modalities
Epididymitis
Introduction
Clinical features
Imaging features
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


