Esophageal Varices
Michael P. Federle, MD, FACR
Key Facts
Imaging
Uphill varices: ↑ portal venous pressure → upward venous flow via dilated esophageal collaterals to superior vena cava (SVC)
Distal 1/3 or 1/2 of esophagus
More common
Downhill varices: Obstruction of SVC → downward venous flow via esophageal collaterals to portal vein and inferior vena cava (IVC)
Upper or middle 1/3 of esophagus
Less common
Fluoroscopy: Tortuous, serpiginous, longitudinal radiolucent filling defects in collapsed or partially collapsed esophagus
After sclerotherapy varices may appear as fixed, rigid filling defects
CECT: Serpiginous periesophageal, gastric, etc.
Enhance as other abdominal veins
Esophageal, coronary ± paraumbilical: Most commonly visualized
Top Differential Diagnoses
Esophageal (varicoid) carcinoma
Thickened, tortuous folds due to submucosal spread of tumor
Rigid, fixed appearance; abrupt demarcation; welldefined borders
Reflux esophagitis,
Submucosal edema may cause thickened folds
Esophageal metastases and lymphoma
Clinical Issues
Esophageal variceal hemorrhage
Accounts for 20-50% of all deaths from cirrhosis
TIPS provides more physiological means of treating varices and ascites
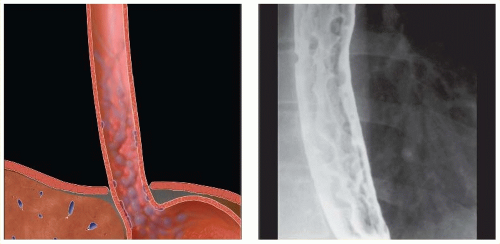 (Left) Graphic shows dilated, tortuous, submucosal collateral veins (varices) within the wall of the esophagus. (Right) Double-contrast esophagram shows tortuous, nodular longitudinal “folds,” typical of varices. These are unusually well depicted, even with the esophageal lumen distended, suggesting that the varices may be thrombosed or sclerosed by endoscopic injection. |
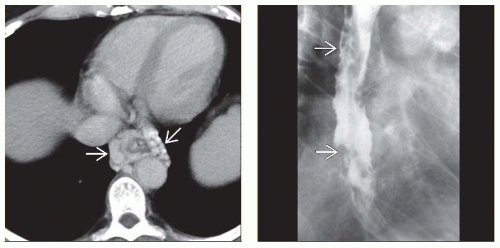 (Left) Axial CECT in a 55-year-old man with upper GI bleeding shows large esophageal varices  . (Right) Esophagram in the same patient, performed after endoscopic sclerosis of the varices, shows fixed filling defects . (Right) Esophagram in the same patient, performed after endoscopic sclerosis of the varices, shows fixed filling defects  in the esophageal wall and lumen. The fixed nature of these mimics the appearance of the “varicoid” morphology of some esophageal carcinomas. in the esophageal wall and lumen. The fixed nature of these mimics the appearance of the “varicoid” morphology of some esophageal carcinomas. |
TERMINOLOGY
Definitions
Dilated tortuous submucosal venous plexus of esophagus
IMAGING
General Features
Best diagnostic clue
Tortuous or serpiginous longitudinal filling defects on esophagography
Location
Uphill varices: Distal 1/3 or 1/2 of esophagus (more common)
Downhill varices: Upper or middle 1/3 of esophagus (less common)
Morphology
Tortuous dilated veins in long axis of esophagus, protruding directly beneath mucosa or in periesophageal tissue
Other general features
Usually due to portal HTN with cirrhosis or other liver diseases
Idiopathic varices: In patients with no portal HTN or SVC block (very rare)
Classification of esophageal varices based on pathophysiology
Uphill varices: ↑ portal venous pressure → upward venous flow via dilated esophageal collaterals to superior vena cava (SVC)
Downhill varices: Obstruction of SVC → downward venous flow via esophageal collaterals to portal vein and inferior vena cava (IVC)
Radiographic Findings
Radiography
Chest radiograph
Retrocardiac posterior mediastinal lobulated mass
± mediastinal widening, abnormal azygoesophageal recess
Fluoroscopic-guided esophagography
Mucosal relief views
Tortuous, serpiginous, longitudinal radiolucent filling defects in collapsed or partially collapsed esophagus
Double-contrast study
Multiple radiolucent filling defects etched in white
Distended views of esophagus
Varices may be obscured
After sclerotherapy varices may appear as fixed, rigid filling defects
CT Findings
NECT
Thickened esophageal wall, lobulated outer contour
Scalloped esophageal mural masses
Uni-/bilateral soft tissue masses (paraesophageal varices)
CECT
Well-defined round, tubular, or smooth serpentine structures
Homogeneous HU; enhance to same degree as adjacent veins
Location
Esophageal, coronary ± paraumbilical: Most commonly visualizedRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree