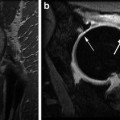
Fig. 9.1
Compression side stress fracture of the left femoral neck
Athletes frequently complain of anterior groin pain that worsens with activity and weight bearing and improves with rest. A stress fracture can be difficult to diagnose since symptoms are often vague [5]. Physical exam may demonstrate antalgic gait or even inability to bear weight on the affected limb [6]. Hip range of motion can be decreased [3]. A hop test, where pain is reproduced with single leg hop, has shown to have increased sensitivity compared to other physical exam findings [5]. However, a hop test should be used cautiously to prevent progression of a stress reaction or cause outright fracture.
Treatment is dependent on the type of fracture. Femoral neck fractures are subdivided into compression (inferior surface, less than 50 % of the femoral neck) and tension (superior surface) types [1, 2, 6, 7]. Compression type stress fractures generally respond to conservative care, with placing the athlete non-weight bearing until asymptomatic and then gradually returning to activity [3, 4, 6]. Conversely, tension-sided stress fractures require surgical fixation due to risk of fracture resulting in malunion, avascular necrosis, and deformity [4, 6]. Any displaced fracture should be considered for urgent surgical fixation [3]. In either type, addressing training factors, biomechanics, and nutritional balance is essential [4]. Return to play may be allowed when an athlete has achieved pain-free range of motion, asymptomatic full weight bearing, and often healing on repeat MRI [7].
Stress fractures in the pelvis, particularly the ischiopubic ramus, can also occur and can present similarly to adductor tendinopathy, osteitis pubis, and athletic pubalgia. Similar to femoral stress fractures, runners have an increased incidence as well as women with the female athlete triad [7]. Recovery and return to sport is often successfully achieved with decreased weight bearing, possibly requiring crutches, and gradual activity progression [7].
True fractures and fracture dislocations of the hip and pelvis, although uncommon in sports, can occur, particularly in contact sports such as football, rugby, and wrestling. Diagnosis is typically not difficult due to the limb deformity and immobility. Appropriate imaging is critical for complete analysis of the injury pattern, and should include AP Pelvis, Judet views, Inlet/Outlet views, and AP and lateral views of the femur. Fractures of the femoral neck, intertrochanteric or subtrochanteric regions, and displaced pelvic or acetabular fractures require urgent surgical management.
Inert Layer
Capsular Injury
The capsule encompasses most of the femoral neck and extends from the intertrochanteric ridge to the acetabular rim. The capsule is then reinforced by surrounding ligamentous and muscular structures. Injury to the capsule can occur in athletic participation or in traumatic hip dislocation [1]. Sports involving axial loading with hip rotation, such as golf, football, and gymnastics, place the capsule at increased risk for capsule stretch or rupture injury [6, 8]. If there is laxity in the hip capsule from previous injury or innate factors, the surrounding soft tissues, such as the iliopsoas muscle, may compensate and become an additional source of anterior groin pain (see iliopsoas tendinopathy below) [6, 9]. Secondary injuries, such as labral pathology, can arise from chronic capsular laxity with resultant suboptimal joint mechanics [9].
Patients generally report anterior groin pain, which worsens with passive external rotation and extension [6]. Treatment is initially conservative with anti-inflammatory medications and physical therapy [6]. If conservative measures are unsuccessful, arthroscopy may be considered for capsular plication [10].
Adhesive capsulitis, while more common in the shoulder, can also be a source of hip pain and decreased range of motion. It may be seen idiopathically, in association with diabetes, or secondary to intra-articular lesions [11]. Similar to shoulder adhesive capsulitis, pathology in the hip is most commonly seen in middle-aged women [12]. Patients often have decreased, painful range of motion, similar to findings in the shoulder [11, 12]. Our experience has been that loss of external rotation is the most pathognomonic feature. However, painful restriction in hip joint motion is a nonspecific clinical finding, and diagnosis can be challenging. Treatment is conservative with range of motion and intra-articular steroid injection, but arthroscopy with manipulation can be considered [11, 12].
Labrum and Femoroacetabular Impingement
Femoroacetabular impingement (FAI) occurs when there is increased contact between the proximal femur and acetabulum, most evident during flexion and adduction of the hip [13]. FAI is the result of anatomical variants of the femoral head–neck junction (CAM), acetabular rim (pincer), or both [14–18]. CAM lesions present as an inclusion injury with increased radius of the femoral head with loss of sphericity, causing shearing over the anteriosuperior acetabular rim and resultant chondral destruction [14, 15, 17, 19]. Pincer impingement is considered an impaction injury and occurs when there is acetabular overcoverage or focal anterior retroversion, which results in labral injury and bone apposition at the acetabular rim [14, 15, 17, 20]. Most commonly, there is a combination of CAM and pincer type impingement [18, 19].
Athletes with FAI often present with gradual onset of decreased range of motion and anterior groin pain, which is worse with prolonged sitting [13, 17, 18, 21, 22]. It is more common in young, active athletes who participate in sports requiring repetitive hip flexion and rotation, such as hockey, golf, martial arts, and dance [15, 21, 23–25]. These movements place the athlete at risk due to the increased stress placed on the labrum during extreme positions. The chondrolabral junction is a vulnerable location for trauma and damage during end range hip movements. When these positions are repeated frequently, the athlete may be at increased risk for early hip osteoarthritis or bone apposition at the acetabular rim, increasing the amount of impingement [20, 26]. Therefore, a careful history regarding training techniques, cross-training activities, hours of training, and sports positions is essential. Pain is reproduced on physical exam with flexion–adduction–internal rotation (FADIR) maneuver [15, 17, 18, 25]. Additional physical exam findings include decreased hip range of motion, particularly to flexion and internal rotation [18, 25].
Initial treatment of FAI involves activity modification with attempt to avoid exacerbated movements and with optimizing the stabilizing hip and core musculature [15, 17, 25, 27]. Anti-inflammatory medications and intra-articular steroid injections may also be considered for diagnostic and therapeutic pain relief [15]. Surgical correction of FAI is often required in high level athletes with the goal to provide increased clearance between the femoral head and the acetabulum [17]. With appropriate postoperative rehabilitation, there have been high rates of successful outcomes in athletes after FAI surgical correction [6]. Importantly, if surgery is considered for other concurrent soft tissue injuries, such as labral tears, it is essential that FAI correction is considered in order to correct the possible underlying etiology [16, 19]. It is important to recognize and treat FAI in athletes as there is often a delay in diagnosis [18] and FAI can be a risk factor for early osteoarthritis of the hip [14, 21, 22, 24, 27].
Some athletes with underlying FAI may be at risk for FAI-induced posterior hip instability [28]. The mechanism of this injury can be non-contact as well as contact and is related to premature anterior contact of the femoral head against the acetabulum with posterior levering of the head out of the socket. This can be associated with a posterior lip fracture, analogous to a bony bankart of the posterior acetabulum, or with posterior capsular stripping off of the acetabulum [28]. A high index of suspicion should be maintained for athletes with continued pain with passive motion after hip injury, as frequently these injuries are mis-diagnosed as simple muscle strains. Loose bodies from cartilaginous or bony fragmentation may be present [28].
FAI is directly related to injuries involving the surrounding hip soft tissue structures, which may become pathological either from underlying abnormalities or from direct mechanical stress [13, 14, 18, 29]. These soft tissue injuries will be dependent on the specific repetitive activity an athlete utilizes for his or her sport. FAI can result in cartilage destruction, labral injury, and compensatory tendinopathies, which will be reviewed in this chapter.
Ischiofemoral Impingement
Ischiofemoral impingement occurs when the quadratus femoris muscle is compressed between the ischium and the lesser trochanter [30, 31]. The psoas insertion and hamstring origin may also be affected. The reduced space can be congenital or acquired, such as after fractures, degenerative arthritis, proximal femoral osteotomy, or total-hip arthroplasty [30, 32]. Ischiofemoral impingement has also been described in conjunction with snapping hip syndrome and has been associated with hamstring and gluteal injuries [33].
Athletes often report buttock pain and medial thigh pain. In some cases, it has been reported to closely mimic hamstring origin pain [33]. Pain can be reproduced on physical exam by placing the hip in extension, adduction, and external rotation [30, 31]. Treatment focuses on optimizing biomechanical forces, and appropriate stretching and strengthening of the quadratus femoris muscle [33]. Guided injection may be beneficial for both diagnostic and therapeutic pain relief. As partial tears have been demonstrated in the quadratus femoris muscle [30, 32, 33]. Surgical resection of the lesser trochanter has been described to provide pain relief, but this population was less active, postsurgical, and older [34], and therefore this larger surgery should be used with caution in younger, active athletes [31, 33].
Subspine Impingement
Subspine impingement occurs when the anterior inferior iliac spine (AIIS) impinges inferiorly on the femoral neck [35–37]. The impingement occurs during hip flexion and results in compression of the AIIS against the anterior femoral neck. It has been associated with avulsion fractures of the AIIS, the origin of the rectus femoris muscle [38], but it has also been described without prior AIIS injury [35–37].
Patients typically report pain with activities requiring repetitive or prolonged hip flexion. Physical examination reveals pain with straight hip flexion and with palpation over the AIIS. Diagnosis can be assisted with intra-articular hip injection resulting in 50 % or greater pain relief to provocative maneuvers [35–37]. Conservative treatment with activity modification, intra-articular injections, and rehabilitation may be sufficient and should be trialed prior to surgical consideration. However, arthroscopic decompression of the AIIS may be necessary and has shown good results in improving function and decreasing pain scores [35–37].
Anterior Muscular Pathology
Rectus Femoris
The hip flexors include the rectus femoris (straight and reflected head) and the sartorius generally occurs at the myotendinous junction. In addition, muscles that cross two joints are at higher risk for strains [39]. Both have also been implicated in apophyseal avulsion injuries in skeletally immature patients [39, 40]. Although relatively rare in the adult population, avulsions of the rectus femoris can occur in the setting of strong eccentric contraction of the direct head. A case report demonstrated a proximal avulsion in two NFL kickers [41] soon followed by a larger NFL survey [42]. Investigators surmise that these injuries occur in kickers going from a hip-extended/knee-flexed starting point to a hip-flexed/knee-extended position. These injuries can be managed conservatively most of the time; however, some studies suggest that operative treatment should be considered in kickers and soccer players. One complication of non-operative treatment is the development of extra-articular impingement due to heterotopic bone formation along the tract of injury, resulting in prominent subspine impingement [36].
Iliopsoas Tendinopathy
The psoas and iliacus muscles originate from the lumbar spine and pelvis, respectively, and combine to insert onto the lesser trochanter where it acts as one of the primary hip flexors [43]. Iliopsoas tendinopathy occurs with repetitive hip flexion movements or hip hyperextension moments [44, 45]. Iliopsoas tendinopathy may occur with iliopsoas bursitis or internal snapping hip (internal coxa saltans).
The iliopsoas bursa, the largest bursa in the body, may become inflamed from internal coxa saltans [2, 43]. This occurs when the iliopsoas tendon rubs over the iliopectineal eminence, anterior femoral head, or anterior hip capsuloligamentous structures [43, 44]. Often there is audible or palpable snapping [2, 43]. Snapping can occur from several mechanisms, but often results from the femur moving from flexion/external rotation into extension/internal rotation and causes the iliopsoas tendon to snap over the iliacus muscle [45, 46].
Patients often present with anterior hip pain or inguinal pain which is worse with activity [43, 44]. They may describe an audible or palpable snap if internal coax saltans is present. On physical exam, there may be tenderness to palpation over the iliopsoas myotendinous junction, pain with resisted hip flexion, positive Thomas test, and pain with FADIR test [43, 44, 47]. Additionally, if internal coxa saltans is present, the patient may have a positive fan test where snapping and pain is reproduced when the limb is moved from flexion/external rotation into extension/internal rotation.
The majority of treatment is conservative and includes correcting muscle imbalances with a targeted strengthening and stretching rehabilitation regime [43–45]. If this alone is ineffective, ultrasound-guided injections into the iliopsoas tendon bursa may be effective [43, 44]. Surgery is rarely indicated, but hip arthroscopy can be considered when all conservative measures have failed [43, 44, 47].
Lateral Muscular Pathology
Abductor Dysfunction
The greater trochanter is the attachment site for five muscles: the gluteus medius, gluteus minimus, piriformis, obturator externus, and obturator internus [48]. Hip abductor dysfunction from chronic overload can result in trochanteric bursitis, gluteus medius/minimus tendinopathy, and snapping iliotibial band (ITB) syndrome [49]. This combination of factors has been grouped into the “greater trochanteric pain syndrome” [49, 50]. Hip abductor dysfunction is more common in women than men, possibly due to the wider female pelvis [48–51] (Fig. 9.2).

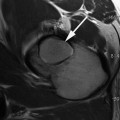
Fig. 9.2
Gluteus medius and minimus tendonosis
Patients typically report lateral hip pain, which is worse with direct pressure, walking, and stair climbing [51, 52]. Back pain is often associated with hip abductor dysfunction, and patients may be treated for lumbar spine pain generators prior to correct diagnosis [50, 51]. Physical exam often reveals tenderness to palpation over the greater trochanter, posterior pain with the flexion–abduction–external rotation (FABER) test, positive Ober test, and weakness with reproduction of pain with resisted hip abduction [48, 51, 52]. A Trendelenburg sign or gait pattern may be present [52].
Most patients respond to conservative treatment and muscle imbalances, particularly including gluteus medius weakness, and should be addressed in any treatment protocol [48, 51, 52]. To facilitate physical therapy participation, decreasing inflammation can be achieved with ice, oral or topical anti-inflammatory medications, or steroid injection [48, 51, 52]. Recalcitrant cases may be addressed with trochanteric bursectomy, with or without ITB release [48, 51]. More recently, platelet-rich plasma (PRP) has been used for the treatment of gluteus minimus and medius tendinopathy and has shown some successes [53] but larger studies are needed. In patients with complete rupture of the tendon insertion or chronic high grade partial tendinopathy that has failed to respond to non-operative measures, surgical repair of the injured tendon can be performed with good and excellent outcomes [54].
Iliotibial Band Dysfunction
ITB syndrome is a cause of lateral hip pain and lateral knee pain in athletes, particularly runners and cyclists [55–57]. The ITB originates from the iliac crest and attaches to Gerdy’s tubercle at the fibular head [57, 58]. Anatomically, it is connective tissue sheath comprising the tensor fascia lata (TFL) and gluteus maximus fascia. ITB pain results from the friction of the ITB over the lateral femoral condyle as the knee moves from flexion into extension [7, 56, 57]. Strength deficits, particularly involving the hip abductors, and increased strain of the ITB are believed to contribute to ITB pain [7, 58, 59]. Additionally, running downhill and running at slower speeds are felt to increase the risk of developing ITB syndrome due to increased friction of the ITB over the lateral femoral condyle [57].
External snapping hip, or external coxa saltans, can be associated with ITB dysfunction [60, 61]. External coxa saltans is most often attributed to the ITB snapping over the greater trochanter [60, 61]. Snapping of the gluteus maximus muscle has also been described [61]. A snap is felt or heard in the lateral thigh and can be accentuated if thickening of the posterior aspect of the ITB or anterior aspect of the gluteus maximus has occurred [61]. The band snaps anteriorly over the grater trochanter from its posterior position as the hip is moved from extension into flexion [60]. External coxa saltans may be one etiology of ITB dysfunction and should be considered during an evaluation for lateral hip pain.
Athletes generally report pain along the lateral hip and thigh, but particularly at the lateral knee [7, 58]. Often, patients report an increase in training regimen, a change in hill running, or a change in footwear prior to development of ITB symptoms. Pain is often worse with activity, particularly running, or shortly after exercise. On physical examination, there is often pain over the ITB to palpation [55]. Ober’s test is often positive and weakness in hip abduction is common [55].
Treatment should be conservative and focus on restoring gluteus medius strength and flexibility imbalances [55]. Decreasing inflammation with ice, anti-inflammatory medications, or steroid injection may also facilitate participation with physical therapy. In some recalcitrant cases that have failed conservative treatments, surgical release may be warranted [56]. Return to running should be accomplished in a gradual, stepwise manner with continued exercises to minimize recurrence [55]. In addition to correcting biomechanics, training factors, such as hills, stairs, and cadence speed, should also be addressed to return the athlete to running.
Posterior Muscular Pathology
Hamstring Tendinopathy
Acute and chronic hamstring tendon dysfunction can affect both professional and recreational athletes. The hamstring comprises the semimembranosus, semitendinosus, and biceps femoris muscles, all originating from the ischial tuberosity with the exception of the short head of the biceps femoris [62–64]. Acute injury is often the result of a sudden eccentric contraction or extreme hip flexion with knee extension [62, 63, 65–68]. Chronic tendinopathy is thought to be the result of mild, low-grade microtrauma, usually from sports such as long-distance and mid-distance running [64, 68].
Both acute and chronic hamstring tendon dysfunctions are most likely to occur immediately adjacent to the myotendinous junction of the long head of the biceps femoris muscle [2, 63, 64]. Athletes typically present with lower gluteal pain or posterior thigh pain that is exacerbated by activity [62, 66]. On physical exam, pain may be elicited by palpation over the ischial tuberosity and bruising or palpable defect may be present in complete or partial hamstring tendon tears [62, 65, 69]. The hamstring acts primarily as a hip extensor and, to a lesser extent, as a knee flexor [62, 66, 70, 71]. Since strength imbalances and poor flexibility are risk factors for both acute and chronic hamstring tendinopathy, restoration and correction of these factors are essential for recovery [63, 66, 68, 71]. Eccentric hamstring strengthening has been shown to be beneficial in preventing new and recurrent hamstring injuries in male soccer players and should be part of any physical therapy program [70]. There is not sufficient evidence to recommend steroid injections into this area. However, preliminary results from our practice suggest a promising role for injection of autologous blood products combined with an eccentric strengthening physical therapy program.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


