Introduction
Venous structure and function are different from their arterial counterparts. Although they both transport blood, the veins perform multiple different functions. Their tasks include transporting blood back to the heart, helping to regulate body temperature and cardiac output, and providing a storage reservoir for blood. Depending on certain conditions, the storage of blood can induce the formation of clots and the possibility of venous thrombosis and pulmonary embolism.
Unlike the examination of the arterial system when the sonologist is focused on arterial stenosis or occlusion, the examination of the venous system requires a different approach. The main goal is to identify or exclude the presence of acute deep vein thrombosis (DVT). Fortunately, duplex and color Doppler imaging is a perfect tool for identifying and evaluating blood clots, thus allowing physicians to take actions to minimize the risks of clot embolization and pulmonary embolism.
To perform venous duplex ultrasound of the veins, the examiner must understand the venous anatomy and be fully acquainted with the examination protocols for imaging the veins. In this chapter we will review the venous anatomy and the examination protocols.
Anatomy of the Lower Extremity
There are three kinds of veins examined by duplex imaging:
- 1.
Deep veins
- 2.
Superficial veins
- 3.
Perforator veins
- •
Vein functions include transport of blood back to the heart, regulation of body temperature and cardiac output, and providing a storage reservoir for blood.
- •
The main goal of the venous duplex examination is to identify or to exclude the presence of acute DVT.
- •
An understanding of the venous anatomy is key to venous examination.
Deep veins
The deep veins are accompanied by an artery and are, by definition, surrounded by muscle. Their job is to act as the main conduits that transport blood back to the heart. Clots within the deep veins are more likely to produce a clinically significant pulmonary embolism because these clots are usually larger than those in the superficial system. Also, because they are surrounded by muscle, the chance of the clot being dislodged during muscle contraction is higher than for a clot in the superficial veins. For these reasons, the main focus in a lower extremity venous duplex examination is on the deep system.
Superficial veins
The superficial veins are, by definition, located near the skin, superficial to the muscle. The main superficial veins usually travel without an accompanying artery within the tissue that separates the fascia from the muscle. Their job is not to be the primary channels for returning blood to the heart, but to get blood close to the skin surface so that the veins can help to regulate body temperature. They constrict when the environment is cold to help preserve body heat. When the body needs to cool down, they dilate to shunt large amounts of warm blood to the skin so that heat escapes from the body.
Although clots within the superficial veins pose less of a threat of producing a pulmonary embolism, clots can and do break loose from superficial veins and travel to the pulmonary arteries. These clots in the superficial system are less likely to cause major, clinically significant pulmonary embolism because they are usually smaller than clots found in the deep veins, and they are less likely to be dislodged because they are not surrounded by muscle. Examination of the superficial veins is still an important part of a complete evaluation of the lower extremity because superficial clots may become large (as the normally small superficial vein is expanded by the contained thrombus) and cause considerable discomfort. There is also potential danger that a superficial vein clot will extend into the deep system.
Perforators
Perforator veins connect the deep veins with the superficial veins. Their job is to keep blood moving from the superficial system into the deep system. When they are working properly, they keep blood from pooling at the level of the skin. When they are not functioning well, blood can pool at the skin level and chronic stasis changes and ulcers may result. Although a complete examination of the lower extremity for the presence of DVT need not include a detailed evaluation of perforators, more attention is paid to them when the question of chronic swelling or venous stasis is being evaluated.
Venous Duplex Imaging Examination Technique and Protocol
The quality of venous imaging studies varies from institution to institution and between individual sonographers. This is related to the lack of standardized training and standardized protocols. Attention to proper technique and following a standardized protocol will increase your likelihood of performing accurate, reliable venous duplex examinations.
There are three factors that will dramatically influence the quality of venous duplex imaging studies:
- 1.
Equipment selection
- 2.
Proper patient positioning and examination techniques
- 3.
Complete standardized imaging protocol
Equipment selection
The quality of imaging equipment varies widely. Attempting venous duplex imaging with inadequate equipment is frustrating and potentially dangerous. The equipment needed for venous imaging will have excellent gray-scale image quality, with the ability to image from the skin line to a depth of at least 6 cm. This may require the use of several transducers: a high-frequency linear probe (10 to 18 MHz) with a small footprint for superficial veins such as the saphenous, distal tibial veins, and most of the arm veins; a midrange linear probe (5 to 9 MHz) for most of the deep veins of the legs and deeper veins of the arm; and a lower-frequency probe (2 to 5 MHz) for the iliac veins and inferior vena cava and also to see leg veins in heavy patients.
Patient positioning for the lower extremity
When imaging the lower extremity, the foot of the bed should be tilted down slightly to allow blood to dilate the leg veins so that they can be imaged clearly. The bed should be placed in a reversed Trendelenburg position (head elevated) at about 20 degrees. Another technique to distend the calf veins is to allow the patient to sit up during calf evaluation. This is extremely effective but is clumsy and can make the veins difficult to compress.
After the bed is tilted, the patient must be positioned properly. Both the patient and the examiner should be as comfortable as possible. For the thigh and calf, this means having the knee slightly bent and the hip externally rotated ( Figs. 18.1 and 18.2 ). This allows full access to the medial portion of the thigh and calf and also allows access to the popliteal fossa. Trying to image the leg without proper positioning will lead to inadequate views and errors in diagnosis.


Patient positioning for the upper extremity
The upper extremity veins are examined with the bed flat and the patient in the supine position. It is especially important that the bed be flat while the jugular and subclavian veins are examined because they will collapse if the head of the bed is elevated. Once these vessels are imaged, the bed can be raised to allow for imaging of the arm veins. The arm is positioned at the patient’s side for examination of the neck veins and the subclavian vein. When examining the axillary veins, the arm is repositioned with the arm extended to allow access to the axilla. It is repositioned again in a slightly lower position with the arm externally rotated to allow access to the medial portion of the upper and lower arm.
Proper technique and diagnostic criteria
Before the 1980s, venograms were the only method available for evaluation of the veins of the extremities. Attempts to image the veins with ultrasound began in the early 1980s. In attempting to find diagnostic criteria for identifying clots, investigators discovered not only that you could see clots on ultrasound, but also that normal veins are so easily compressed with light probe pressure that vein compression could be used to determine unequivocally the absence of thrombus in that vein. Defining compression of the vein as the primary criterion for duplex imaging for DVT was the major factor in its universal acceptance. Using compression in this way allows for the examination to progress quickly in a transverse plane to evaluate the extensive venous anatomy.
Imaging normal, thrombus-free veins
Most of the imaging during the venous duplex examination is performed in a transverse plane with gray-scale images. The vein and its accompanying artery (if a deep vessel) are identified alongside each other. The artery is thicker walled but usually the smaller of the two (if the limb being examined is positioned below the heart). Light probe pressure is exerted directly over the vessels. The thicker-walled artery will resist compression (as it is under higher pressure). The vein should compress easily. If there is any confusion about which vessel is the artery or vein, the examiner should use Doppler to distinguish completely and accurately between the two structures before proceeding.
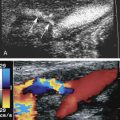
If the vein is thrombus-free, it will compress completely so that the inner vein walls actually touch each other. When the vein collapses completely with light probe pressure, it can be determined to be unequivocally thrombus-free at that location ( Fig. 18.3 ). This is the key to venous duplex imaging of the veins. The pressure on the vein is released, and the vein will reopen. The examiner then moves the probe along the length of the vessel until the entire vein has been imaged in this way. It is important to ensure that these compression maneuvers are as close together as possible. If the cuts are too far apart, a major section of vein containing thrombus can be missed. As a rule, the smaller the cuts, the less chance there is of missing a thrombus. Color Doppler can be used to help visualize the veins in the transverse plane. Care must be taken to evaluate for compression with gray scale because color signals can obscure thrombus. Augmentation of the distal extremity also aids in the visualization of the veins and to demonstrate patency (discussed later).


After the entire segment of vein has been evaluated in the transverse plane, the examiner can rotate the probe and rescan the segment in the longitudinal plane with color and pulsed Doppler ( Fig. 18.4 ). These views provide additional information regarding blood flow through the venous system. These longitudinal views, however, are in addition to the information already gathered by the transverse compression views and cannot substitute for them.

Color and Doppler information added to transverse compression views
Current accreditation protocols require transverse compression views and longitudinal views with color and pulsed Doppler information to be performed at specific levels. Doppler signals in the normal leg vein will be phasic (suggesting the absence of obstruction of the major veins above the level of the probe). Blood flow in the vein should stop completely as the patient takes a breath in and should resume spontaneously as the patient exhales. Squeezing the leg distal to the level of the transducer should produce an augmentation of flow during this maneuver ( Fig. 18.5 ). This indicates the lack of an obstruction of the major veins below the level of the transducer to the level of the squeeze. The examiner must understand the limitations of information gathered by pulsed or color Doppler; a partially obstructive thrombus may be missed using these methods, thus there is a need for transverse compressions.

Determining the presence of thrombus
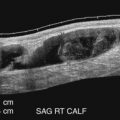
Thrombus is present within the vein when echogenic material is identified within the lumen of the vein ( Fig. 18.6 ) and when full compression of the vein cannot be obtained. It is crucial to note that both of these things must occur together to make a definitive diagnosis of thrombus in the vein ( Fig. 18.7 ). Some laboratories simply look for noncompressibility of the vein or echogenicity in the vein lumen to make the diagnosis of DVT. Failure to link these two will result in false-positive results in cases where the veins are difficult to compress, not because of the presence of thrombus but because of a myriad of other factors. For example, proximal compression of the vein by pelvic mass or adenopathy, causing stagnation and increased echogenicity of blood flow, may simulate intraluminal thrombus. Complete compression of the vein lumen excludes thrombus ( Fig. 18.8 ). Other pitfalls include incomplete compression from a patient bearing down in response to painful probe compressions ( Fig. 18.9 ), poor patient positioning, compression being limited by a nearby bone, and other factors. In the case where the vein is not compressible but thrombus cannot be seen directly (poor views or views of very small or deep structures), an additional maneuver is essential to determine whether the lack of compressibility is because of the presence of thrombus or some other factor. This additional maneuver may involve compressing harder until the artery next to the vein starts to compress. If the artery next to the vein compresses and the vein does not, thrombus is likely to be present within the vein despite the fact that the clot is relatively anechoic or is not directly visualized. Augmentation of flow through the noncompressible segment may also demonstrate patency, although this maneuver may not exclude a partially occlusive clot. If there is uncertainty regarding the presence of DVT, a correlative study with magnetic resonance venography or computed tomographic scanning may be required for further evaluation .
- •
The main focus in a lower extremity venous duplex examination is on the deep system because the chance of a clot embolizing to the lungs is higher than for a clot in the superficial veins.
- •
Clots in the superficial system are less likely to cause major, clinically significant pulmonary embolism because they are usually smaller than clots found in the deep veins, and they are less likely to be dislodged because they are not surrounded by muscle.
- •
Three factors that influence the quality of venous duplex imaging studies are equipment selection, correct patient positioning and examination techniques, and complete standardized imaging protocol.
- •
Normal veins will compress completely so that the inner vein walls actually touch each other.
- •
Visualization of intraluminal thrombus and incomplete compression of the vein are the primary criteria for duplex imaging for DVT.
- •
Present accreditation protocols require transverse compression views and longitudinal views with color and pulsed Doppler information to be performed.
- •
Thrombus is present within the vein when echogenic material is identified within the lumen of the vein and when full compression of the vein cannot be obtained.
- •
Incomplete compression of the vein may be caused by pelvic mass or adenopathy, the patient bearing down in response to painful probe compressions, poor patient positioning, compression being limited by a nearby bone, and other factors.




The Venous Anatomy and Examination Protocol
Start at the groin crease
Examination of the lower extremity veins usually begins at the groin crease ( Fig. 18.10 ). Just above the crease, the main venous trunk is called the external iliac vein. As it crosses the groin crease, it becomes the common femoral vein ( Figs. 18.11 and 18.12 ).



Common femoral and large saphenous veins
The common femoral vein gives off a superficial branch just below the inguinal ligament ( Fig. 18.13 ). This is the large saphenous (great saphenous) vein ( Fig. 18.14 ). This vein had been called the greater saphenous vein. The great saphenous vein ( Fig. 18.15 ) travels (close to the skin line) down the medial aspect of the thigh ( Fig. 18.16 ) and eventually continues in the anterior medial calf all the way into the foot ( Fig. 18.17 ).





After the great saphenous vein unites with the deep system just below the inguinal ligament, the common femoral vein continues as a single trunk accompanied by the common femoral artery until it bifurcates to form the femoral (superficial femoral) and deep femoral (profunda femoris) veins ( Fig. 18.18 ).

Femoral vein (superficial femoral) and deep femoral vein (profunda femoris)
The names of these veins (femoral and deep femoral) continue to create confusion. The vein previously called the superficial femoral has recently been renamed the femoral vein because many people would hear the term superficial femoral vein and confuse it with the great saphenous vein, which is a superficial vein. The vein previously called the profunda femoris is now called the deep femoral. In this text, we will use the updated names: the superficial femoral vein will be called the femoral vein, and the profunda femoris will be called the deep femoral vein. Just remember: the femoral vein is the main deep vein that runs through the thigh.
The femoral vein courses down the thigh alongside the femoral artery ( Figs. 18.19 and 18.20 ) with the deep femoral vein deeper in the thigh. The femoral vein is bifid or duplicated in about 25% of patients ( Fig. 18.21 ). It continues down the thigh, serving as the primary route of venous drainage until, at the proximal end of the adductor canal, it dives deep and becomes the popliteal vein.